Saloni@salonium
Hepatitis B is a tiny virus with just 4 genes.
But it kills hundreds of thousands globally per year, mostly by infecting babies and causing liver disease or cancer over the following decades.
In a new episode of HARD DRUGS, we tell the story of the hepatitis B vaccine, which became the first of many milestones:
It was the first viral protein subunit vaccine, the first recombinant vaccine, and the first vaccine to prevent a type of cancer.
Key stats:
• Hepatitis B virus has just 4 genes, some of which overlap, making it one of the most genetically compact human pathogens
• It has a very unusual life cycle for a DNA virus: it forms a stable mini-chromosome (cccDNA) inside liver cell nuclei, and uses reverse transcription, similar to HIV.
• It integrates itself into your liver cells' DNA, causes repeated cycles of cell damage and repair, and inflammation that eventually leads to cancer.
• During infection, the virus produces ~500 quadrillion (5 x 10¹⁷) copies of its surface antigen in the bloodstream. They act as decoys, soaking up our antibodies and helping the virus evade immunity, and it sticks around in our cells for decades.
Over time, it causes one of the most common and deadliest liver diseases and cancers:
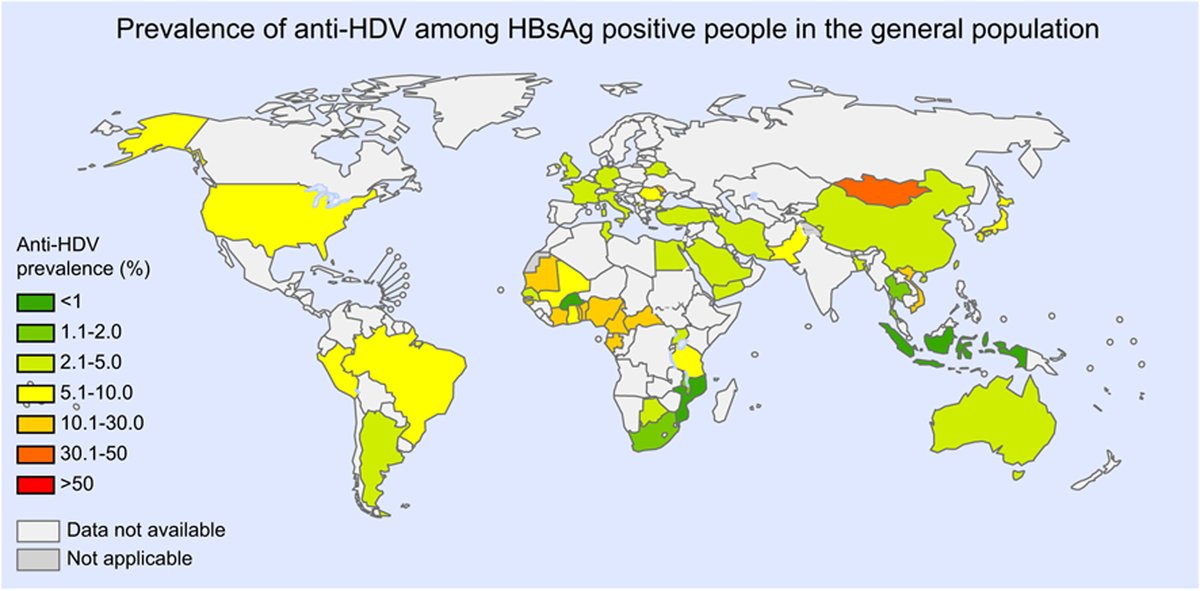
~300 million people worldwide are living with chronic hepatitis B
~600,000 people die from hepatitis B each year, mostly from cirrhosis and liver cancer
While only ~5–10% of adults infected develop chronic infection, ~90% of infants infected at birth do. Around a third of those infants will eventually die from liver failure, cirrhosis, or liver cancer.
But there's a vaccine against it: the hepatitis B vaccine. It is so efficient that it helps us block the virus by training us to recognize just one protein (the surface antigen) quickly, before it can overwhelm us.
The first hepatitis B vaccine (1981) was made from human plasma, through multiple brutal inactivation steps that kill other microbes and contaminants.
The second hepatitis B vaccine (1986) was the first recombinant DNA vaccine ever, made by factories of yeast cells churning out the antigen in bulk.
The payoff has been enormous. Large cluster randomized trials have shown that hepatitis B vaccination reduces liver cancer rates by 85% and deaths by 70%.
Universal vaccination of newborns has led to massive drops in hepatitis cases, liver failure, and liver cancer in younger generations.
As the first viral protein subunit vaccine, it was built upon a series of breakthroughs in immunology, advances in virology and vaccinology.
In this episode, we trace the discovery of hepatitis, hepatitis B virus, the development of vaccines, and their impact.
And we explore how we even got to subunit vaccines at all: the great battle of immunology, the discovery of antibodies and their incredible diversity, and how that understanding could be used to test, study, and build better vaccines.
If you want to understand how modern vaccines actually came to be, or why hepatitis B vaccination still matters today, this one’s for you.
Timestamps:
0:00:00 Introducing the hepatitis B vaccine
0:15:46 The mysterious trail of jaundice outbreaks and the search for an invisible liver pathogen
0:28:03 How a tiny virus causes cirrhosis and liver cancer, and the struggle to identify it
0:53:19 How Maurice Hilleman developed the safest, purest vaccine in history
1:17:36 Turning the hep B vaccine recombinant
1:29:14 The impact of hep B vaccination
1:39:27 How we got here: the 19th century battle for the soul of immunology
2:01:34 How the body builds an infinite library of defenses
2:19:25 Why scientists thought immunology was solved in the 1960s
2:30:57 How better immunology led to precise subunit vaccines
2:45:33 Conclusion