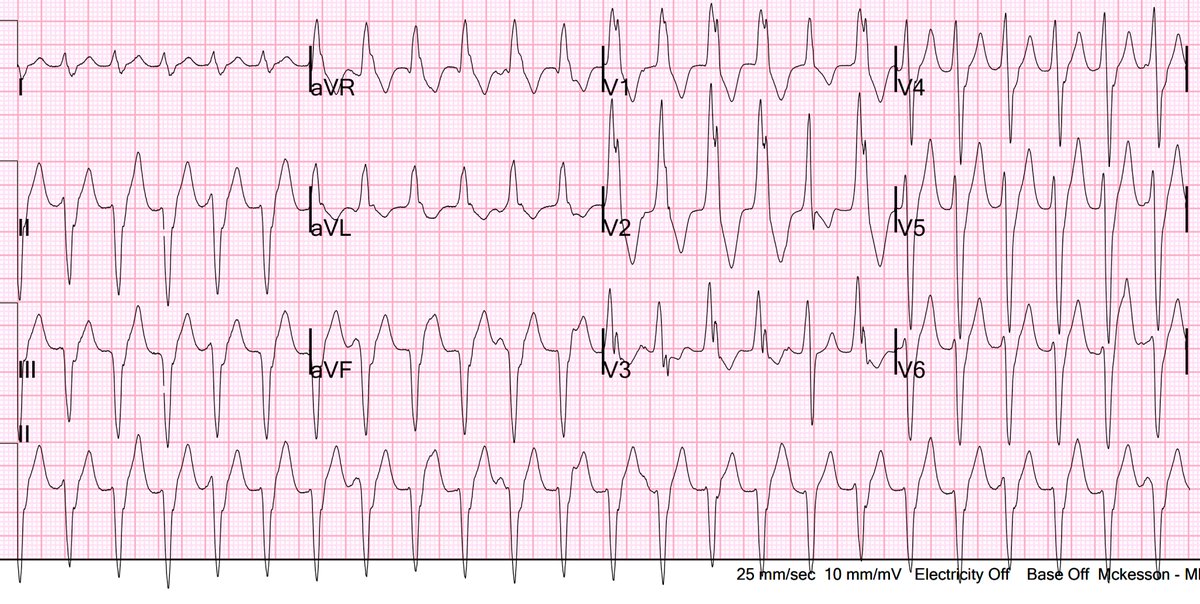
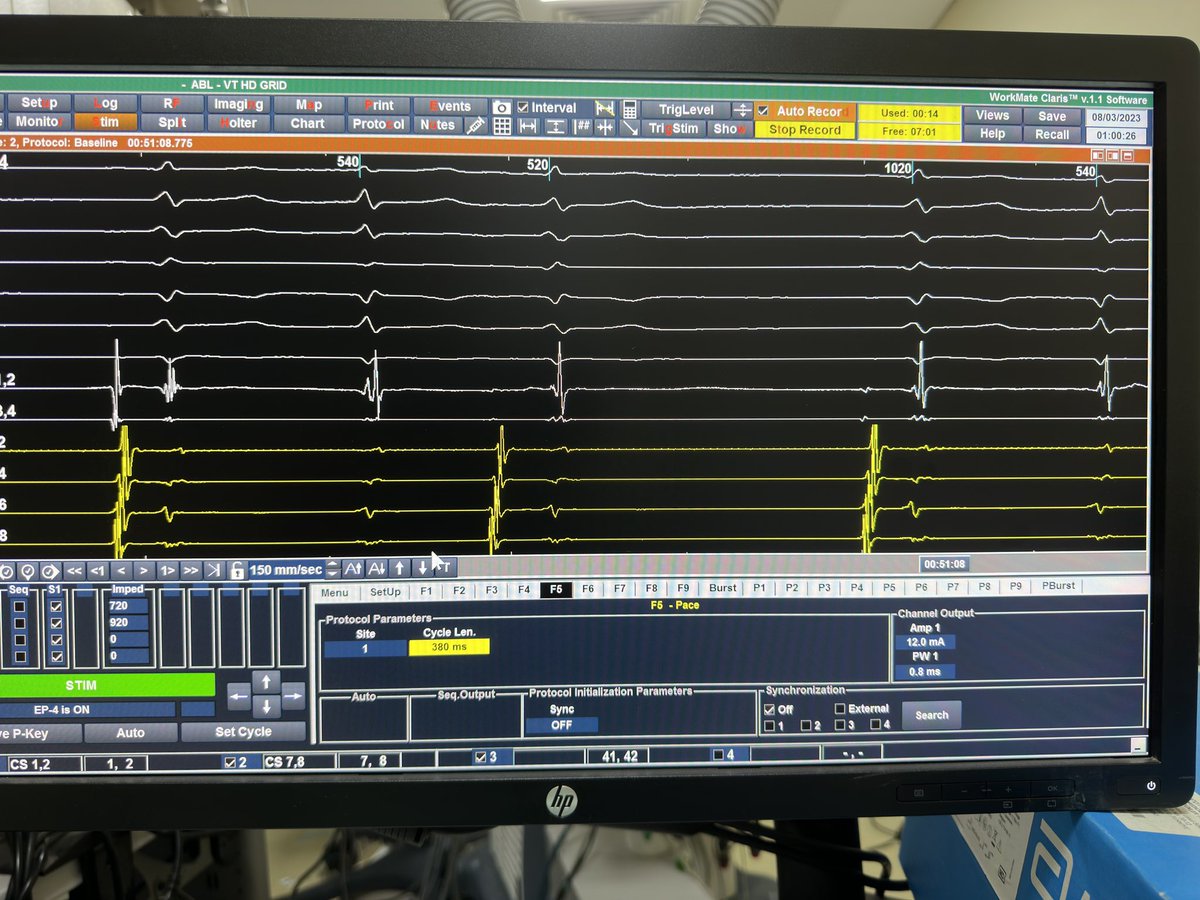
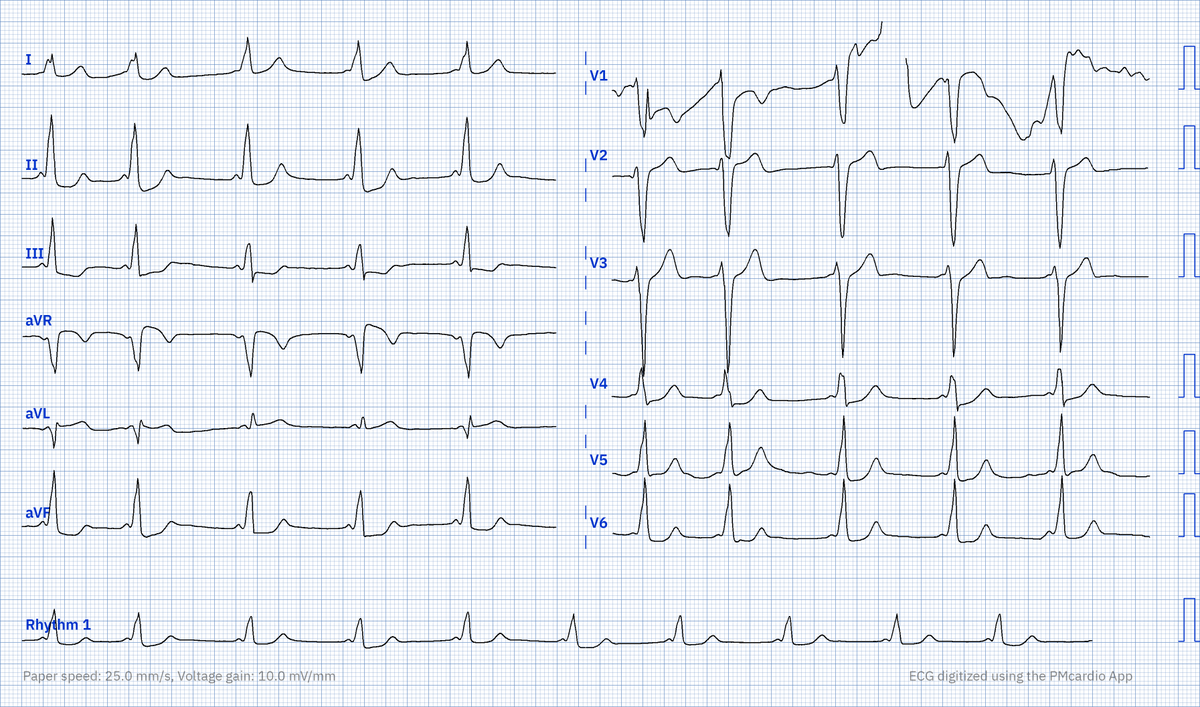
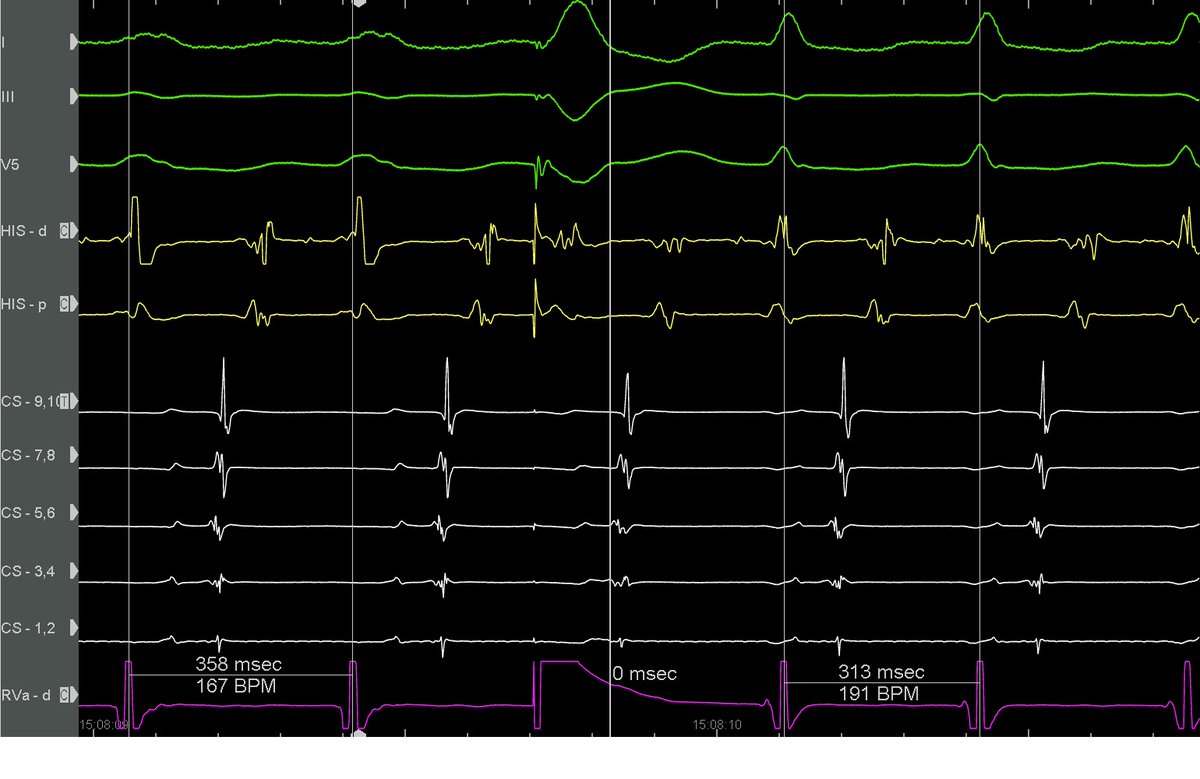
Lovely classical EP case. BCT on Holter and on arrival in the lab. What observations can you make from this single screenshot?
English
Charlie Pearman
44 posts
@CPearman_EP
Cardiologist. Electrophysiologist. Inherited Cardiac Conditions enthusiast. But mainly just a Dad.