Sabitlenmiş Tweet

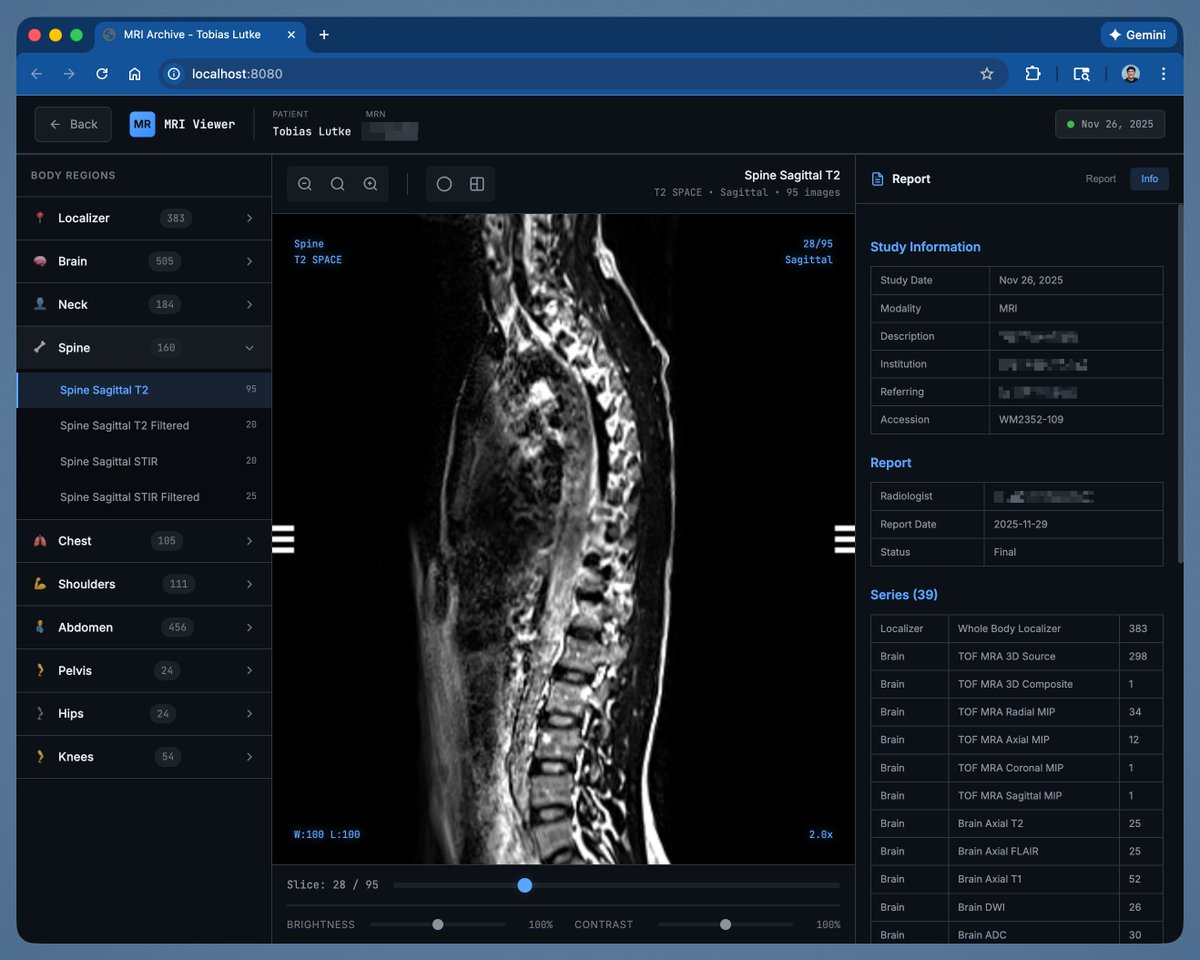
Where is the best place in the U.S. to have a whole-body MRI wellness screening? Grok’s answer: MRIatbelfair.com

English
A. Joseph Borelli, Jr., MD
29.2K posts

@DocBorelli
🩻 Radiologist & MRI clinic owner | Chaired committee writing U.S. MRI accreditation standards | Filmmaker | All tweets IMO | No investment/medical advice




One of the simplest things for humans, but incredibly complex for machines, is anticipating the unpredictability of children. Here FSD rolls up in direct sun, spots the kid way before I did, and applies the brakes. But what came after stunned me. Another bike, and another, then a gap, and another bike (and a bonus scooter). At no time did FSD attempt to jump the gap between the children (even when it could have). There was no jitter or indecision. FSD just patiently waited until they all came around the corner and crossed the street. It stayed perfectly still so as not to scare the children. Just like a human would. I’ve seen a lot of amazing things with FSD, but this one really impressed me on a deeper level. As a father, I’m happy knowing more people are using Tesla FSD to keep their own kids safe and to ensure the safety of the kids on the road.











In 2019, Elon said HW3 was enough for Full Self-Driving. Seven years later, it needs to be Supervised by a human due to safety concerns. Tesla calls it Full Self-Driving Supervised, because they know it will make dangerous maneuvers at any given moment.
Samsung Foundry’s Principle Engineer has announced that “the @Tesla-Samsung Al5 chip has reached tape-out. It is scheduled to be manufactured at the Taylor fab using our latest 2nm process and will soon be integrated into Tesla's newest products.” Volume production won’t start for a while, but good to hear things are still moving along. Picture of Tesla’s upcoming AI5 chip on the right:

Model YL HW5 next year? 👀

