Robert Pfeffer retweetledi

Fair point about ARPI! I don't fully agree.
To be clear, I am talking here about low-volume mHSPC.
Few points:
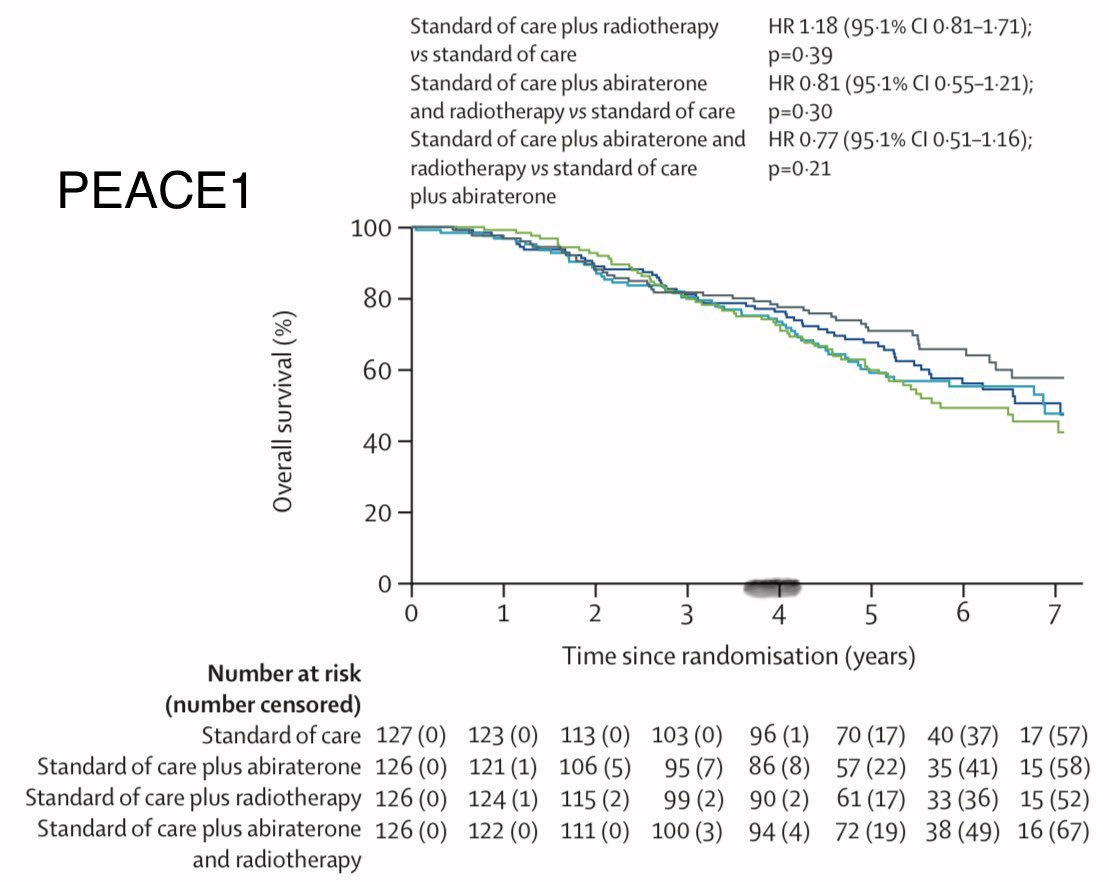
1- I wouldn't say PEACE-1 showed no OS benefit. It doesn't prove a benefit, neither does it disprove one. HR for SOC+Abi +/-RT was 0.77 (Curves below). There is certainly a trend. I think we need a higher N for the ARPI subgroup. There was however a signicant improvement in CRFS.
2- In a NMA (@soum_roy_radonc) with Bayesian pairwise comparison, the best treatment was SOC+ARPI+RT, and was associated with reduced mortality wrt SOC+ARPI
europeanurology.com/article/S0302-…
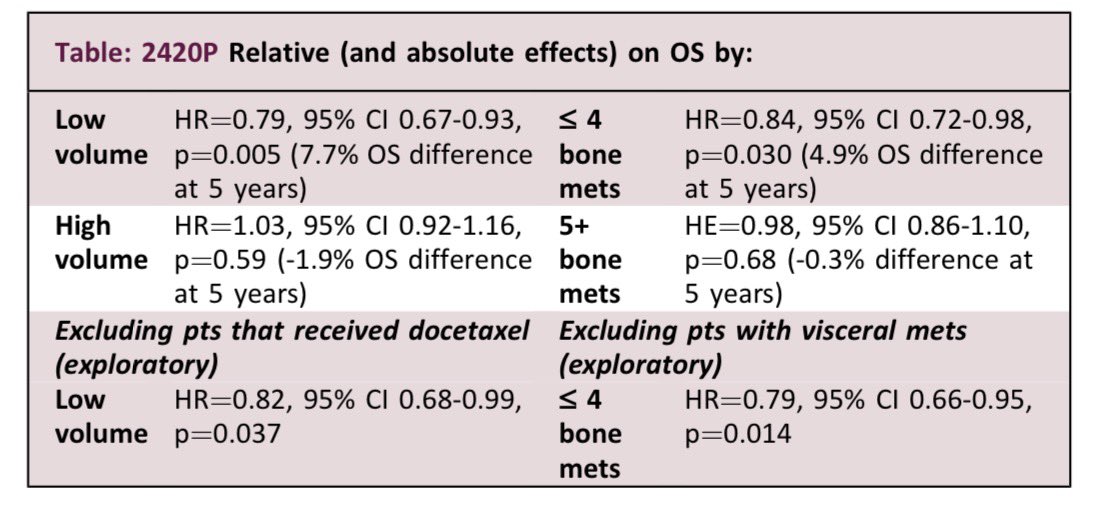
3- STOPCAP meta-analysis (including PEACE-1 data) showed an OS HR of 0.92 (0.84-1.0) for RT for all-comers, low and high-volume (Forest plot below). For low-volume, OS HR was 0.79 (0.67-0.93).
annalsofoncology.org/article/S0923-…
urotoday.com/conference-hig…
So based on the above, I think it's safe to say that RT to the primary is beneficial for low-volume mHSPC treated with ADT +/- ARPI. PEACE-1 cannot rule out an OS benefit for the ADT+ARPI subgroup, mainly due to small N and Frequentist design. It does however prove a CRFS benefit. On another hand, a Bayesian comparison (NMA above) showed that these patients most likely benefit from RT.
In light of these, I think it's hard to NOT recommend RT even with ARPI. Wondering what is the current practice at your institution. Also curious to know what other Rad-Onc colleagues think about this
@pcaparker @soum_roy_radonc @drspratticus @tylersbrt @seanmmcbride @sbrtsean @alison_tree @vedangmurthy @piet_ost @paulsargos @jryckman3 @5_utr @adib_elio @protonstorey @docpriyamvada @_shankarsiva @albertobossial @amarukishan


English