Sabitlenmiş Tweet

We’re officially live!
Get The Ultimate Asset here
Your playbook for how to dominate midlife and beyond
a.co/d/hUjS9AU
English
Sandeep Palakodeti, MD MPH
9.1K posts

@DrDeepMD
Author, The Ultimate Asset: https://t.co/ZL9EcEU5DO. Physician, CEO & Founder @join_velocity ex- @harvardmed @mayoclinic

🇺🇸 Brett Blackman, owner of a healthcare software company, just got convicted in a $1 BILLION Medicare fraud conspiracy. His platform auto-generated fake doctors’ orders and prescriptions to scam Medicare and other programs out of over a billion dollars. The DOJ literally coded the fraud at industrial scale. Guilty. Source: U.S. Dept. of Justice

@john_malone It’s not malpractice when all the professional society guidelines say to prescribe after a 2 (at best 9) question survey that basically anyone would test “positive” for on any moderately tough day “But judge, that’s what the gUiDeLiNeS say” Case dismissed

⚡️The real signal is credential deflation. MBA demand is falling because the market is finally separating elite network access from generic credential theater. The top MBA still has value because it buys access: elite peers, recruiting funnels, status compression, VC/startup networks, private equity pipelines, consulting/IB placement, alumni power, and social sorting. That part survives because the product is not just education. It is access to a protected human network. Everything below that is getting exposed. A huge amount of MBA value was built on the idea that business knowledge was scarce. It is not scarce anymore. Basic finance, strategy, marketing, ops, accounting, management frameworks, case studies, memo writing, market analysis, valuation, and presentation structure can now be learned or generated faster, cheaper, and more directly through AI, YouTube, work experience, online courses, and actual operating reps. The credential moat is cracking. This connects directly to the broader white-collar quake. AI is attacking the value of generalized cognitive packaging. A mid-tier MBA used to signal polish, ambition, managerial readiness, and business literacy. Now the market is asking a colder question: What can this person actually do? Can they sell? Can they build? Can they operate? Can they allocate capital? Can they lead? Can they use AI to produce leverage? Can they own a result? The paper matters less when the work product becomes visible. Business schools are being hit by the same force hitting software agencies and white-collar labor: the collapse of artificial scarcity. When knowledge, frameworks, decks, models, and analysis become abundant, the value shifts to judgment, network, trust, execution, taste, distribution, and real-world outcomes. That is why tuition cuts matter. Price is truth. When schools slash tuition, they are admitting the old willingness-to-pay broke. The deeper cultural signal is brutal: the professional-class bargain is weakening. For decades, the advice was: get the degree, buy the credential, enter the managerial class, rise safely. That path worked when credentials controlled access to information, employers, and status. AI and labor-market saturation are breaking that bargain. The winners will be elite institutions with network power and operators with proof of work. The losers will be expensive middle credentials selling generic knowledge. The real truth: The MBA is splitting into two products. At the top, it remains a status-and-network asset. Everywhere else, it is becoming overpriced business school cosplay in a world where AI can teach the frameworks and the market wants proof you can actually move reality.

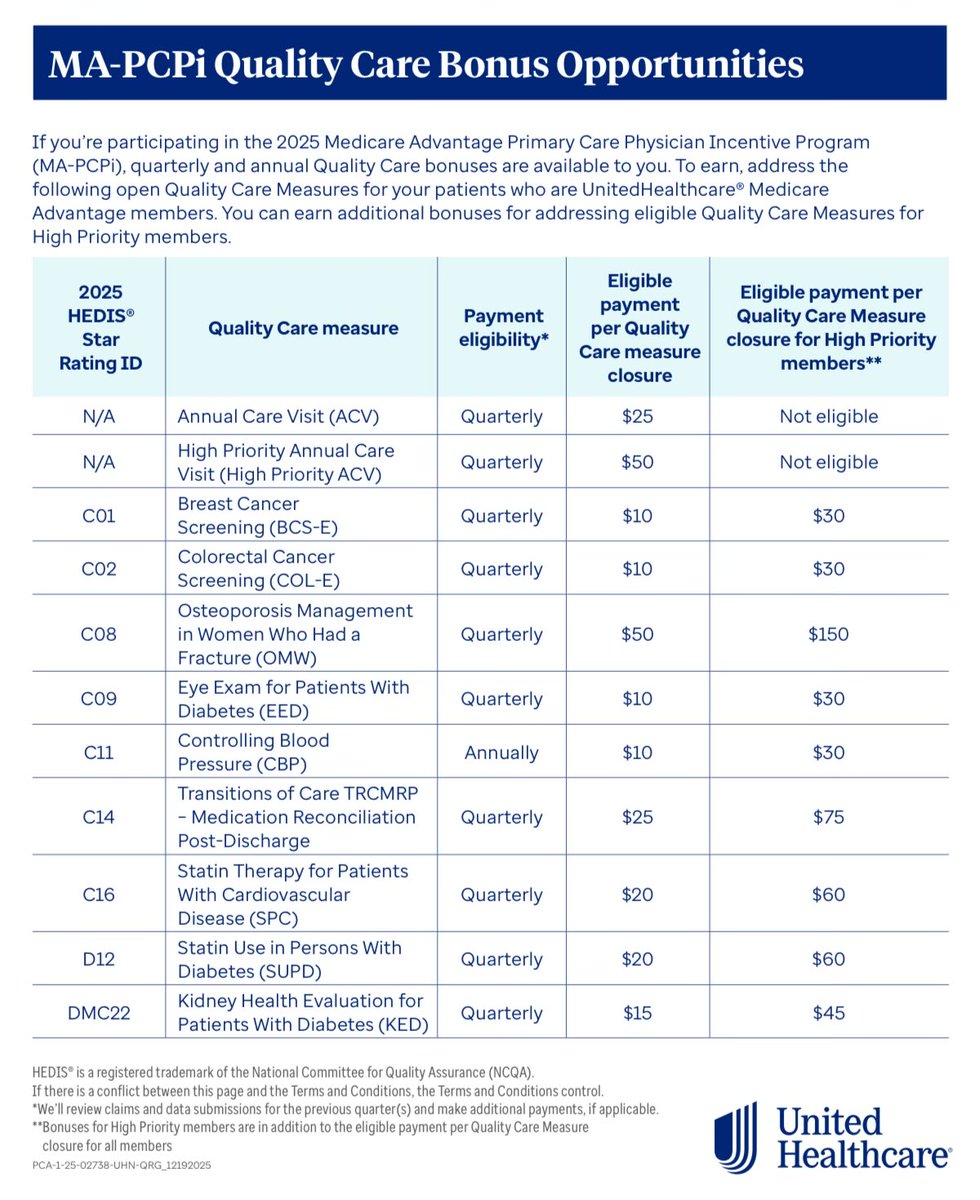


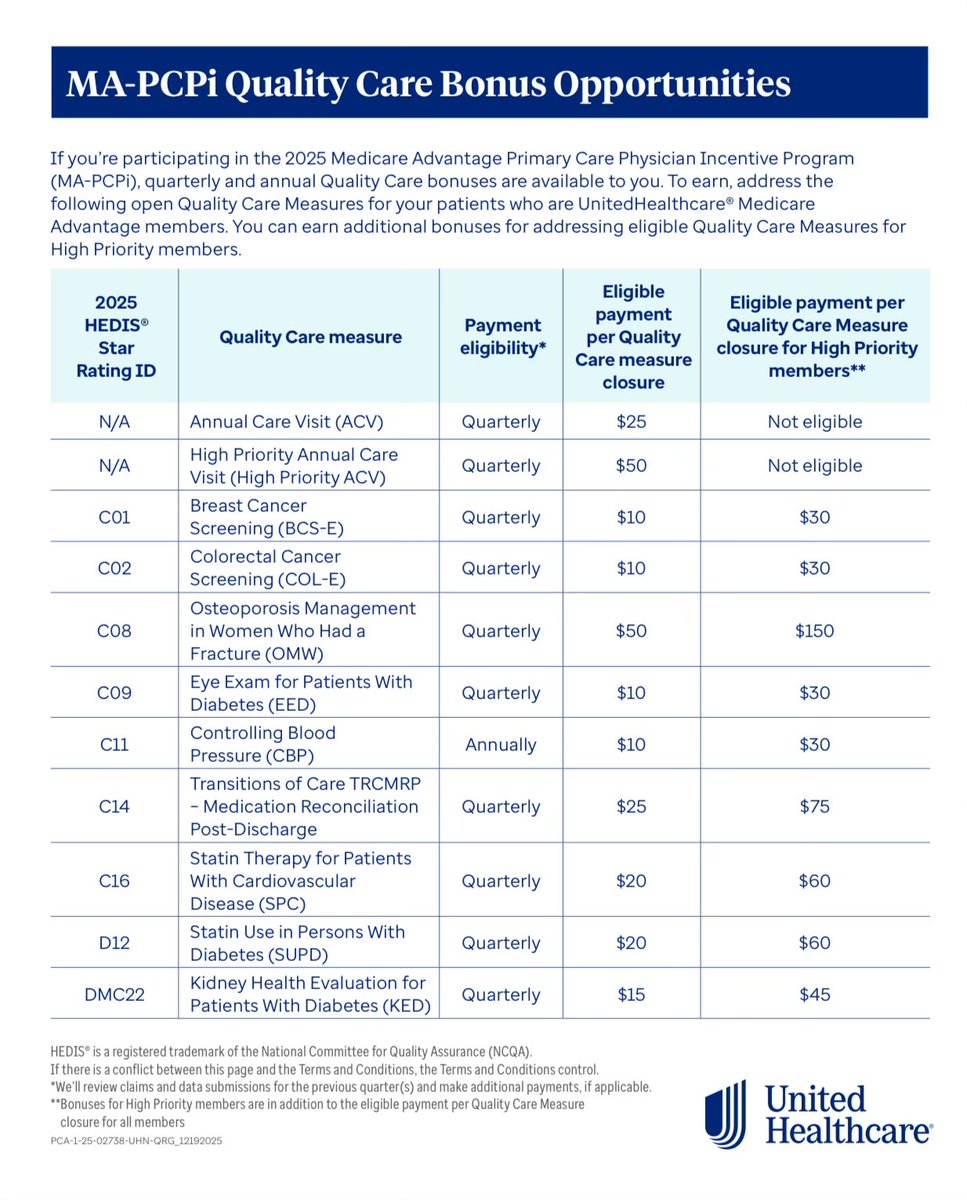
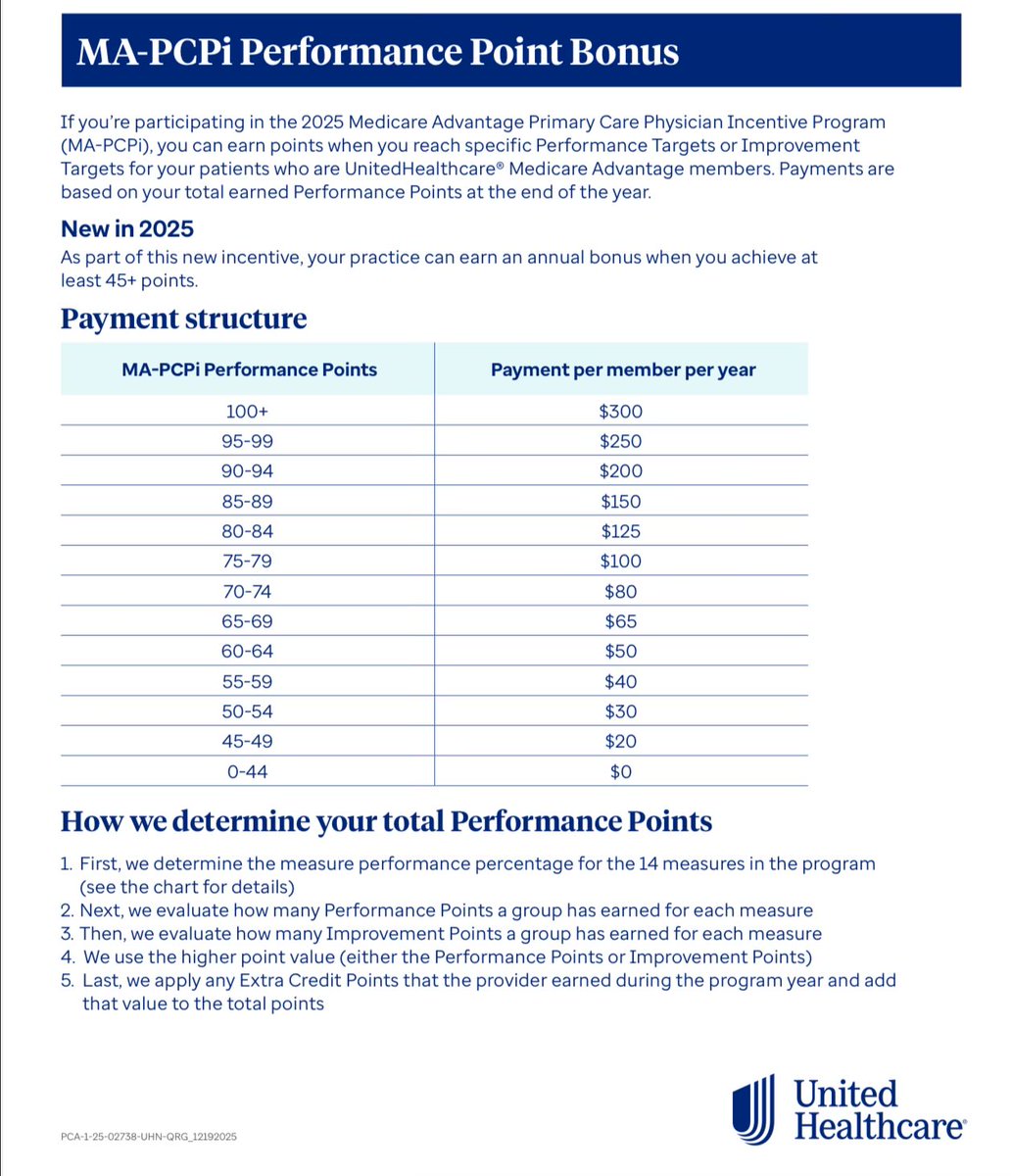
And no the docs aren’t getting paid by pharma to prescribe But here’s how the flow of funds works: Pharma puts pressure on professional societies to create guidelines a certain way —> payors take guidelines and operationalize into incentive structures —> health systems want that extra $$ and to be seen as “high quality” to the public —> they bonus docs for meeting thresholds on their panels —> patients get put on meds —> pharma has recurring revenue for life 82% of docs are employed by a corporate entity. It’s so easy to see how we got here if you just follow what drives the world in every other industry. And this is why @SecKennedy considering RICO charges for collusion at the top level. And why it’s so important to find an independent physician who reports to no one but YOU the patient. It’s all one big club. And we ain’t in it. Godspeed and good luck out there

1 in 3 college aged kids being on psych meds is absolutely bonkers We’ve completely lost the plot


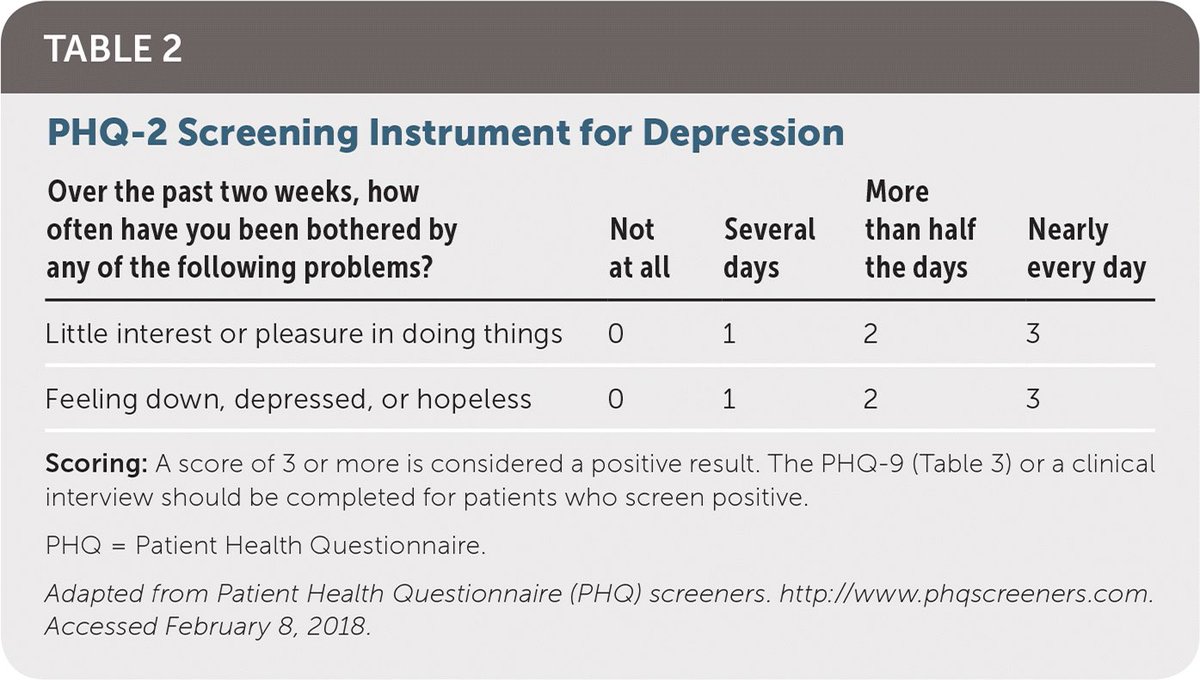
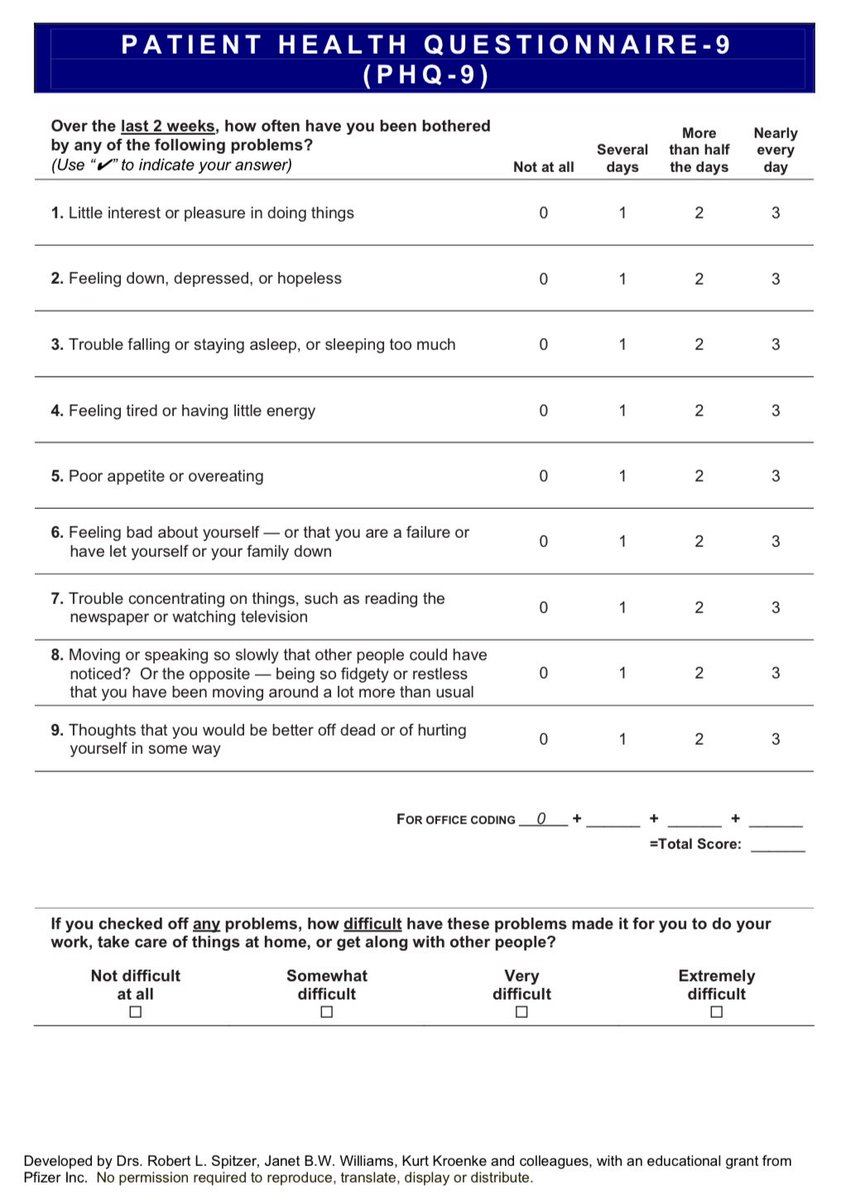
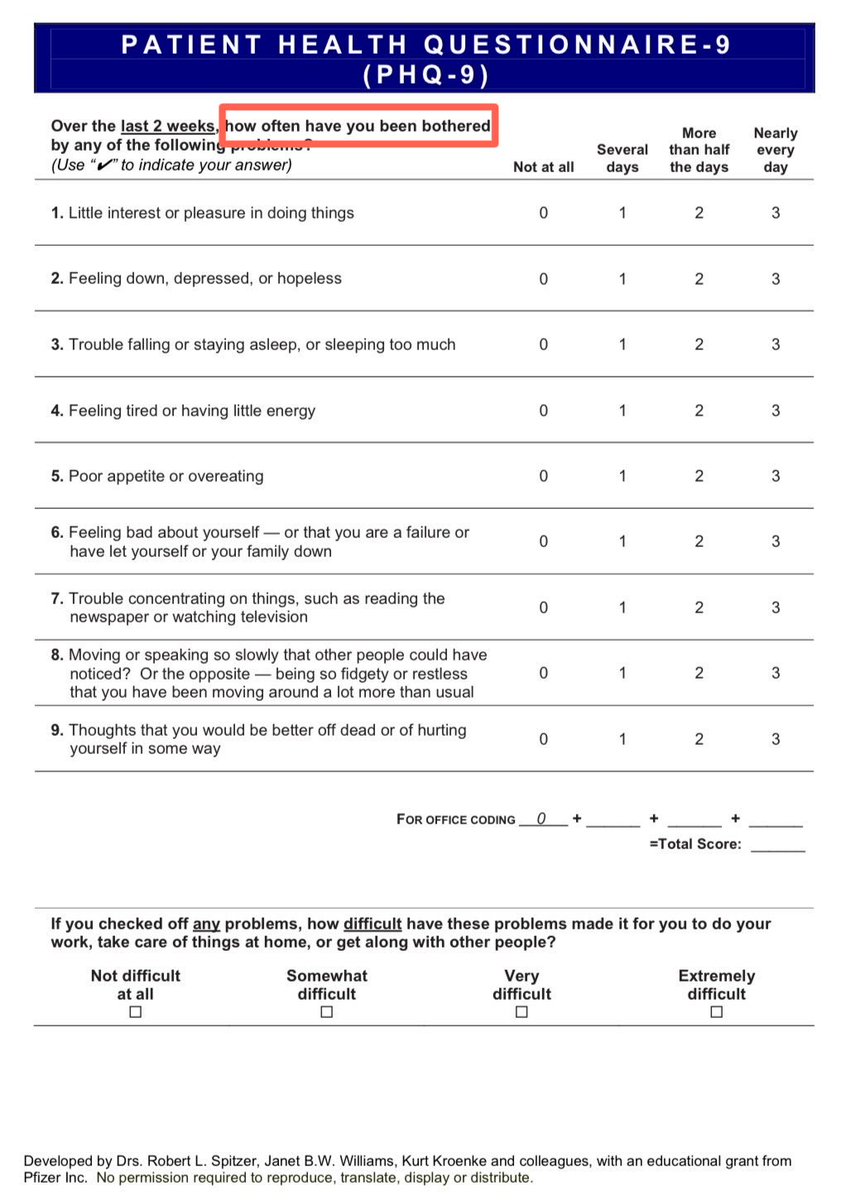
Let me explain how this works in real life A PHQ2 score is collected on almost every patient that walks in the door of a primary care clinic. At best, a PHQ9 Posted both here for your viewing pleasure TWO questions asked ONE time and MDD is “likely”. 9 questions seals it
Let me explain how this works in real life A PHQ2 score is collected on almost every patient that walks in the door of a primary care clinic. At best, a PHQ9 Posted both here for your viewing pleasure TWO questions asked ONE time and MDD is “likely”. 9 questions seals it
“Roughly 1 in 6 American adults, an estimated 44 million people, are now on antidepressants. In young adults, those numbers are even higher. Thirty percent of college students take psychiatric medication, up from 9% in 2007.” wsj.com/opinion/behind…