Sabitlenmiş Tweet

Hemodynamics and Right Heart Cath tweetorials collection.
All in one place!
Threads:
1. PA Catheter (PAC 101). The basics
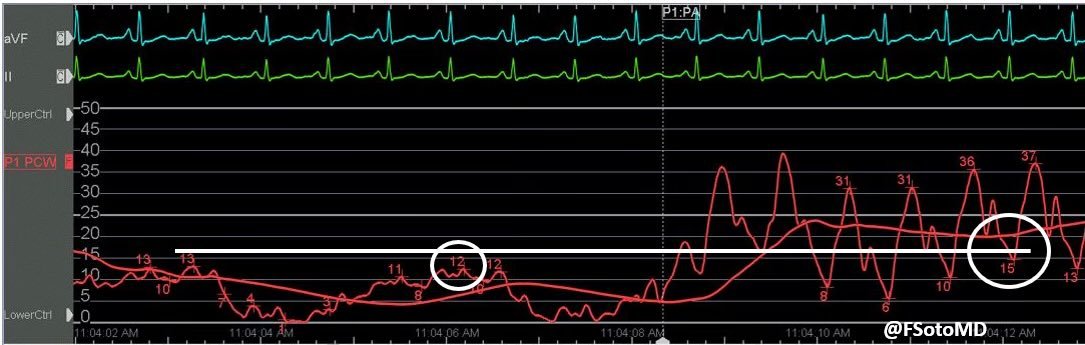
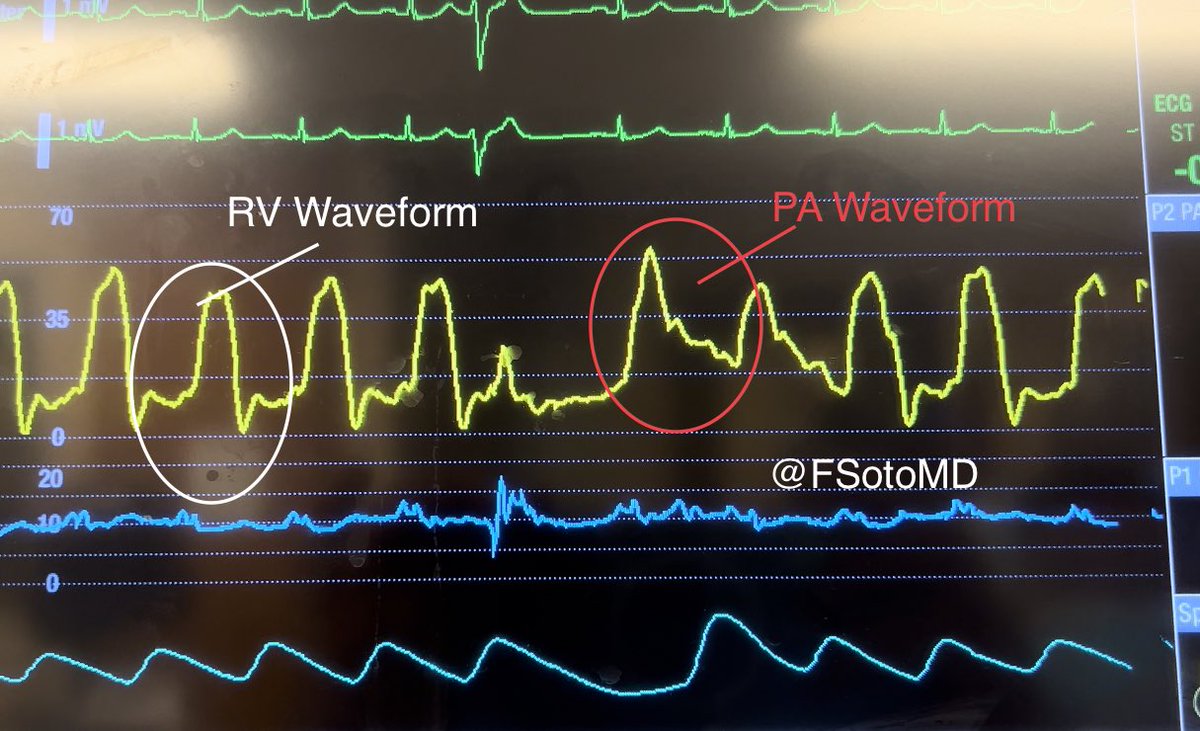
2. Waveform recognition (PAC in ICU)
3. Quality control: 🔑troubleshooting before you use the data
4. Preventing the most dreadful PAC complication
English