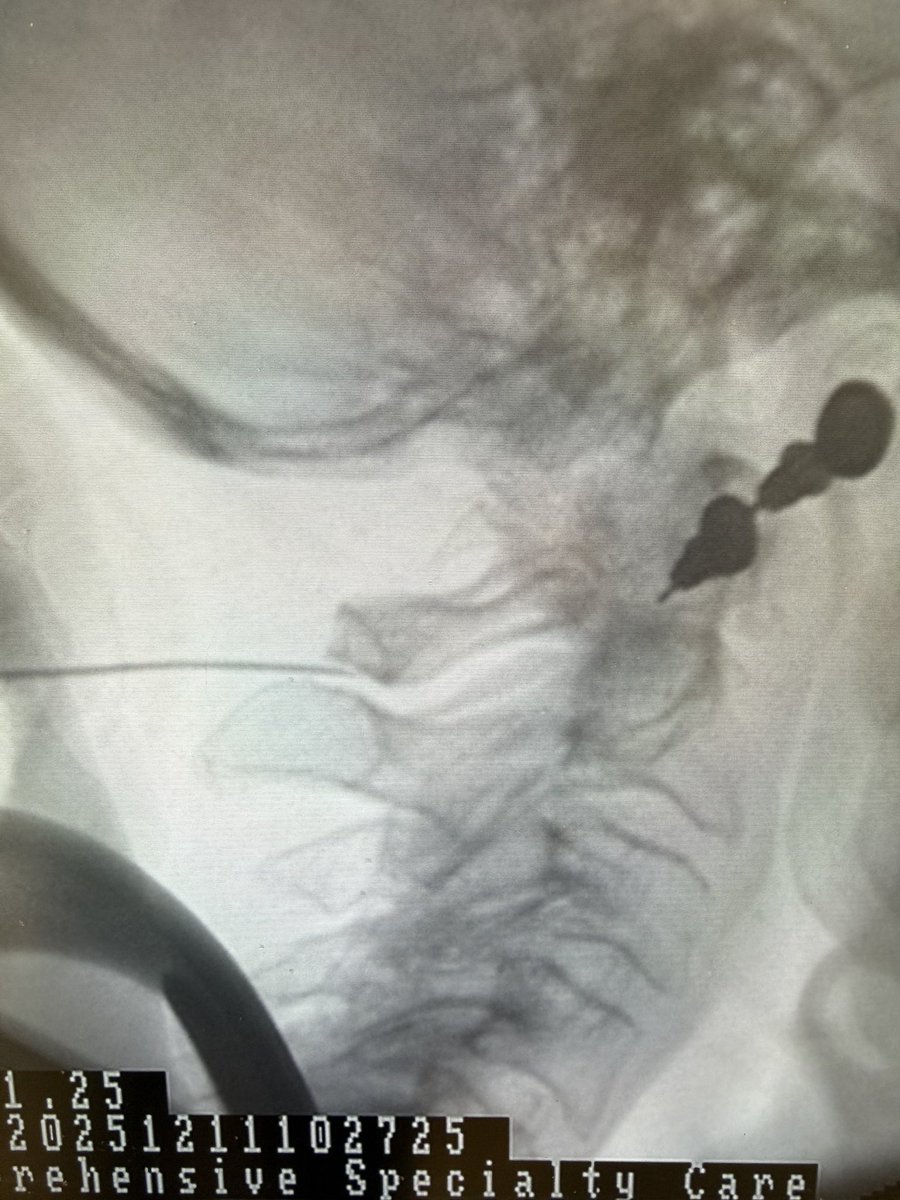
Interesting case of C1 – 2 interspinous bursitis treated with an injection of local anesthetic and steroid anti-inflammatory. Very effective treatment in this case.
@jkhmlf Yes. Auto=self i.e. self fusion (without hardware). Some call it spontaneous fusion but I think that that is a misnomer. There’s not really much spontaneous about it, it’s due to a process occurring over years if not decades.
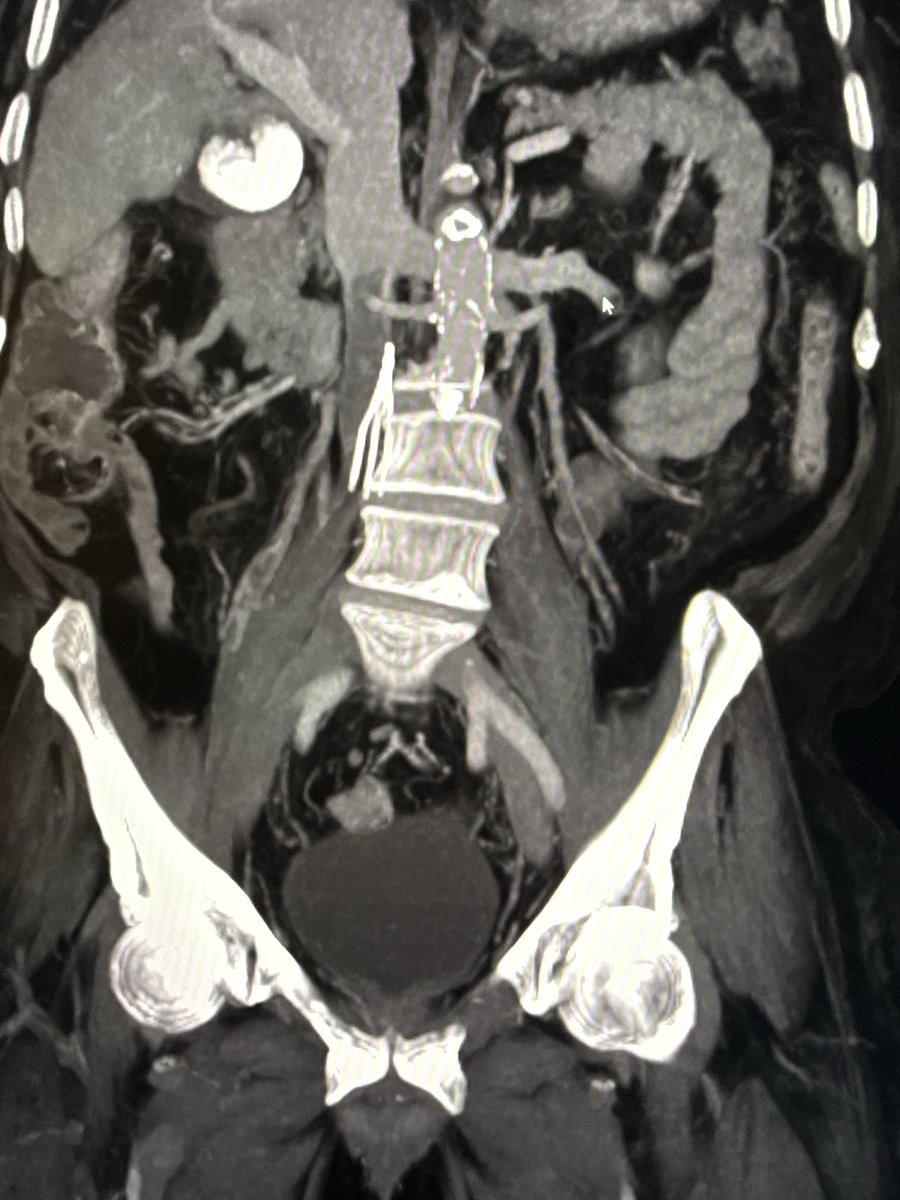
Radiologists: please be sure to mention autofusions on cross-sectional imaging studies. This typically indicates a seronegative spondyloarthropathy. That was the case in this patient with neck pain but no mention on the radiology report.
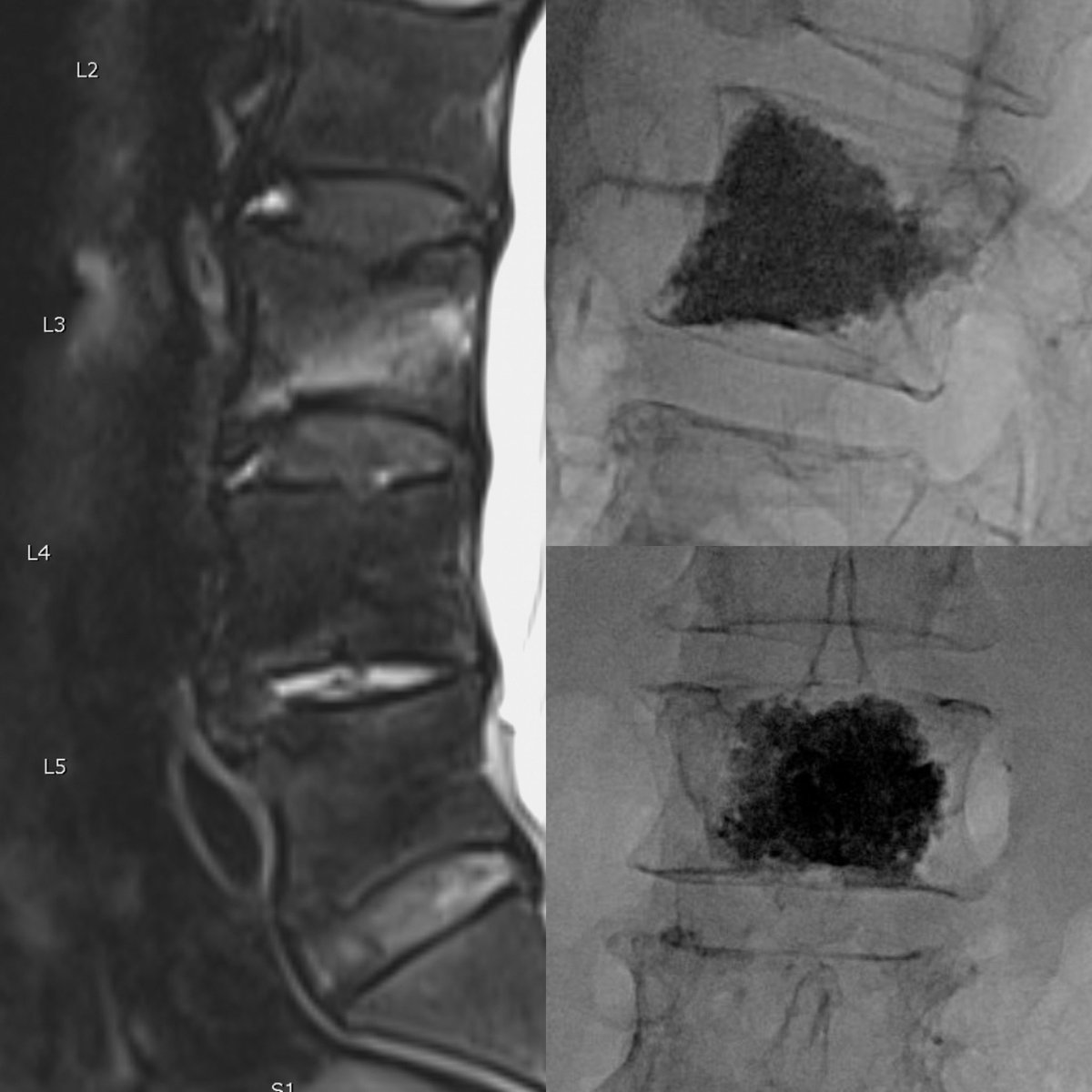
Aetna health insurance making up criteria for denying #kyphoplasty for a very painful and debilitating vertebral fracture. See #6…there’s no such contraindication or medical literature basis for denying kyphoplasty for a fracture extending through the posterior vertebral cortex
Just released! Stay up to date on the latest insights, education, and advancements shaping the field of interventional spine.Grab your copy now: aspnpain.com/aspn-newslette…
@doctdeer @Scorah_ssmb
Tarsal Tunnel Syndrome: An Ultrasound Pictorial Review
doi.org/10.1002/jum.15…
Tarsal tunnel syndrome (TTS) is an entrapment neuropathy caused by compression of the posterior tibial nerve or its branches as they pass beneath the flexor retinaculum at the medial ankle. Clinical presentation is often nonspecific, including burning pain, paresthesia, numbness, and discomfort worsened by activity or at night. Diagnosis is challenging because symptoms can mimic other conditions, and conventional tests such as the Tinel sign and plain radiographs lack specificity.
High-resolution ultrasound has emerged as a key diagnostic tool because of its accessibility, low cost, and superior spatial resolution compared with MRI. It allows dynamic and comparative studies, identification of nerve compression sites, and evaluation in weight-bearing positions. Ultrasound can also help differentiate causes, guide interventions, and complement electrophysiological testing.
Etiologies of TTS are varied and include bone and joint abnormalities (such as hindfoot valgus, coalitions, spurs), accessory ossicles, synovitis, rheumatoid arthritis, and post-traumatic changes. Expansile lesions like ganglion cysts, lipomas, and nerve sheath tumors are also implicated. Metabolic conditions such as diabetes, gout, hyperlipidemia, and hypothyroidism can predispose to nerve enlargement or compression. Muscular causes include hypertrophy or supernumerary muscles (accessory soleus, accessory flexor digitorum, peroneocalcaneus internus). Tendinopathy, tenosynovitis, vascular abnormalities, and iatrogenic factors like surgical hardware or scarring are additional contributors.
Conservative management includes rest, anti-inflammatory therapy, orthotic support, and physiotherapy, with surgery reserved for refractory cases depending on the underlying pathology. Awareness of the diverse causes and ultrasound findings is essential to ensure timely diagnosis, prevent morbidity, and improve patient outcomes.
#POCUS#ultrasound#ecografia#ankle
Anterior Chest Pain: Differential Diagnosis
A 19-year-old rugby player developed anterior chest pain 36–48 hours after participating in a weekend tournament, which did not prevent him from continuing his sporting activity.
An initial X-ray and ultrasound were performed, which revealed no abnormalities. A chest wall MRI was completed, revealing physiological absence of closure at the level of the first sternal crest (between the second and third sternebrae) associated with subchondral irregularity at its ends, moderate adjacent bone edema, and minimal posterior subperiosteal edema. A chest CT scan revealed a minimal increase in the junction between the first and second segments of the sternal body, associated with minimal soft tissue enlargement posterior to the sternal body. These findings are consistent with instability at the level of the first sternal crest.
During embryological development, the sternum forms from six cartilaginous precursors called sternebrae. The first forms the manubrium, the second to fifth the body, and the sixth the xiphoid process. The bony fusion of the sternal body segments is complete by age 25, so during adolescence, they develop a fibrous union that can be unstable after trauma.
Treatment is conservative, and measures include limiting sports activity, oral anti-inflammatory treatment, and physical therapy.
@ChengaziMD Very much what I was going for. Goal is enough internal fixation to allow for eventual bony fusion around the segment. Given pt's propensity to form bone, hopefully should work. Important to fix any adjacent level fractures that could compromise stability; luckily T8 already done
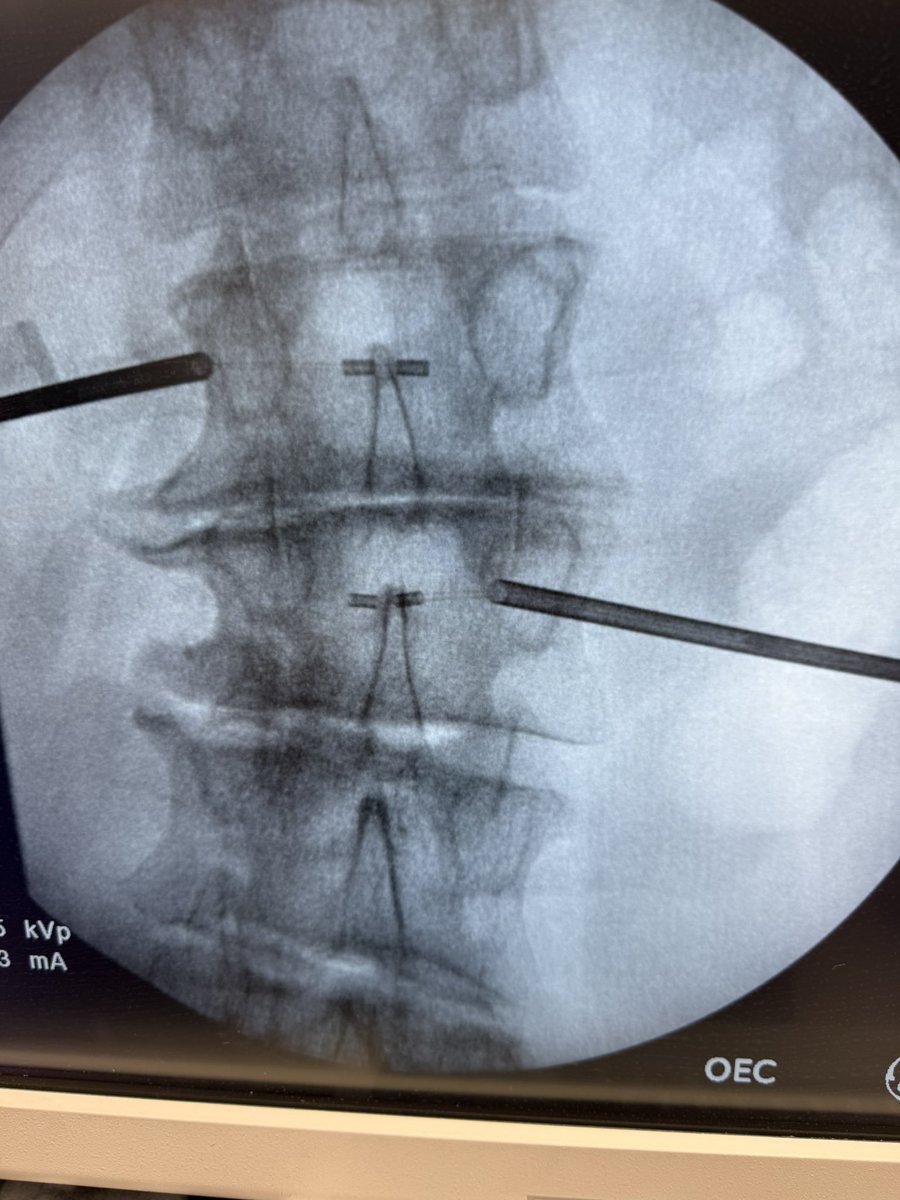
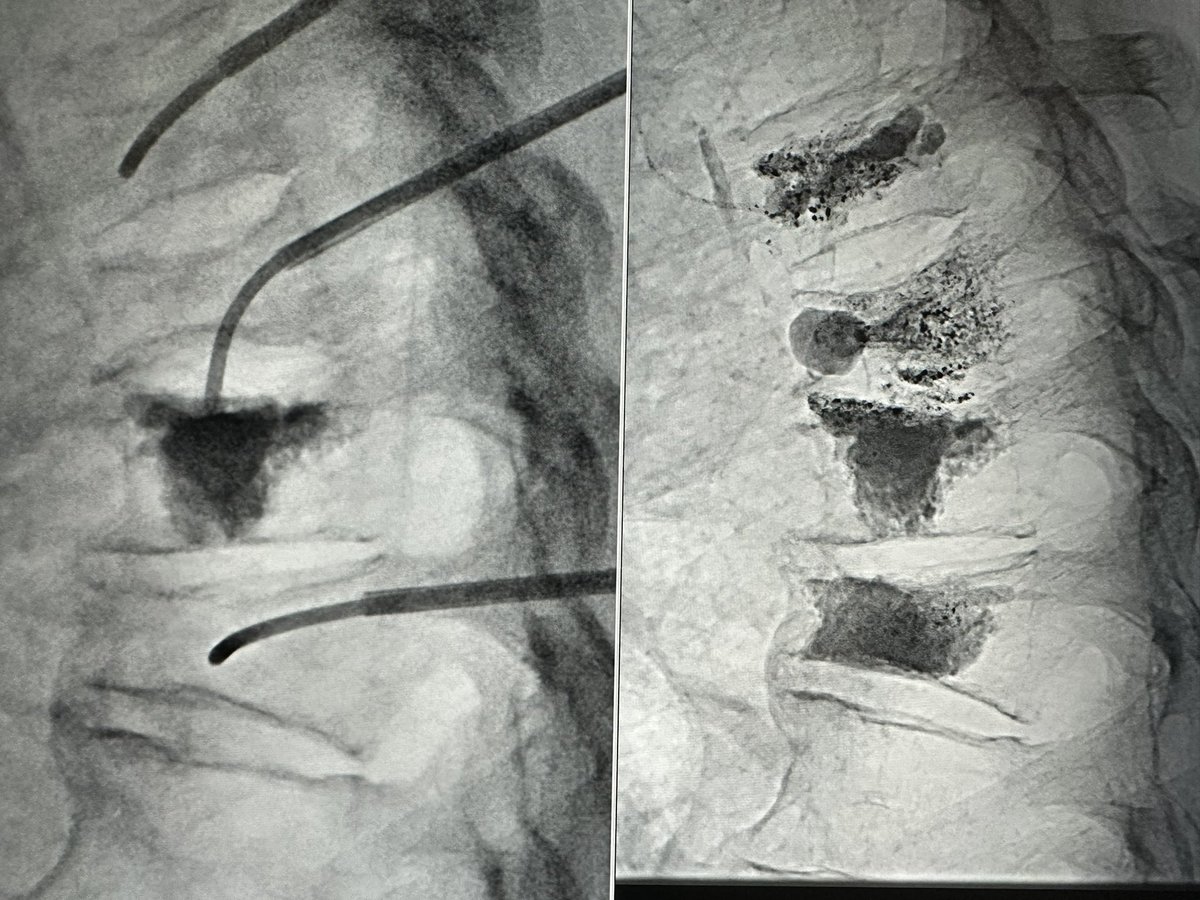
Sometimes controlled extravasation is beneficial. T10 and recurrent T9 fracture s/p T8,9 kypho previously. Fracture morphology complicated by DISH. Transpedicular disc access for T9 kypho and discoplasty to consolidate osteophyte and endplate. Ugly, but effective. #disasterplasty
Curved needles and cement cannulas are helpful for targeting focal fracture clefts. Small T8 superior endplate cleft after otherwise sufficient kypho at OSH was not amenable to pedicular access. Transdiscal access from above made for an easy fix.
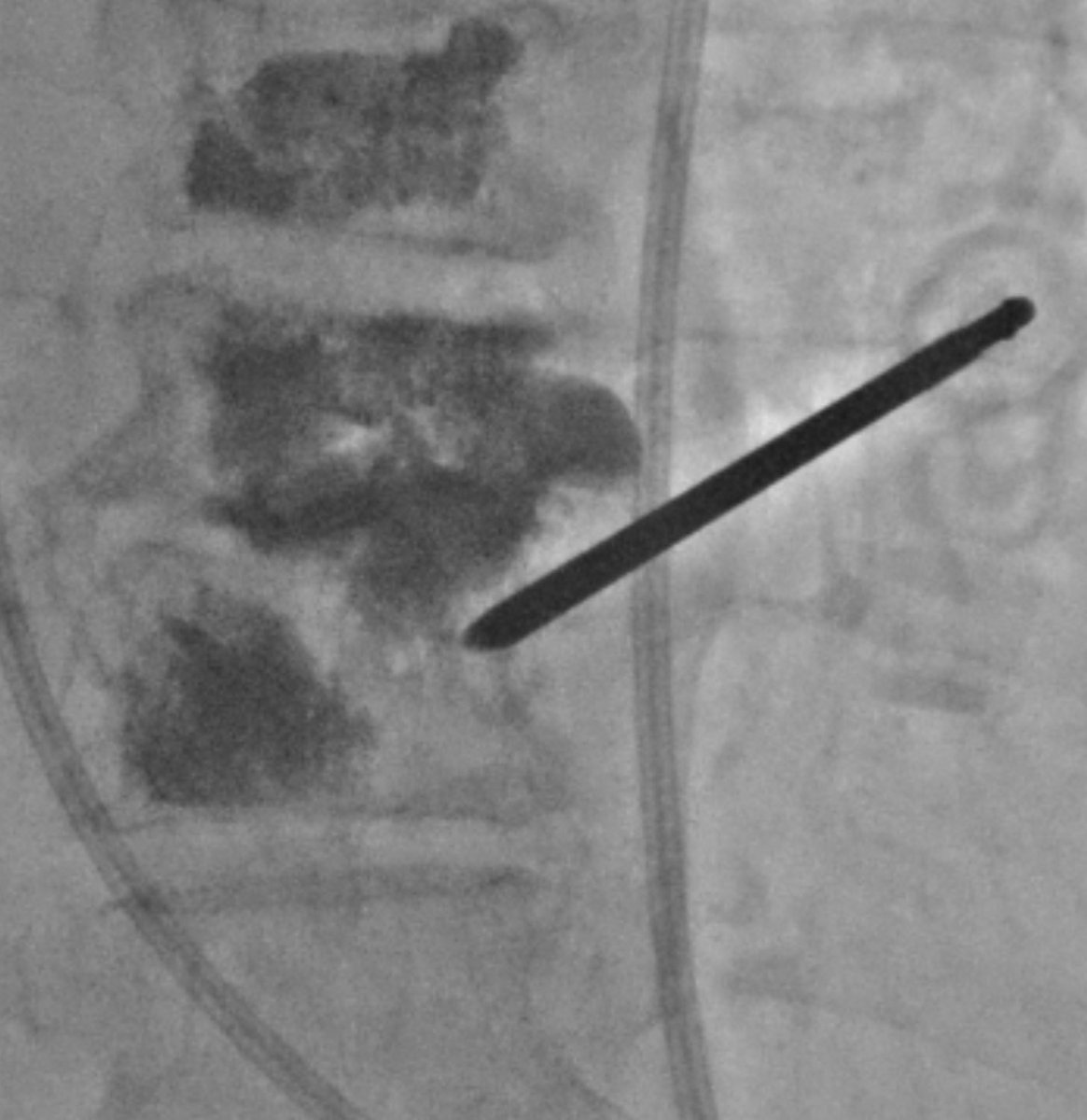
(4/4) A bit more cement and done.
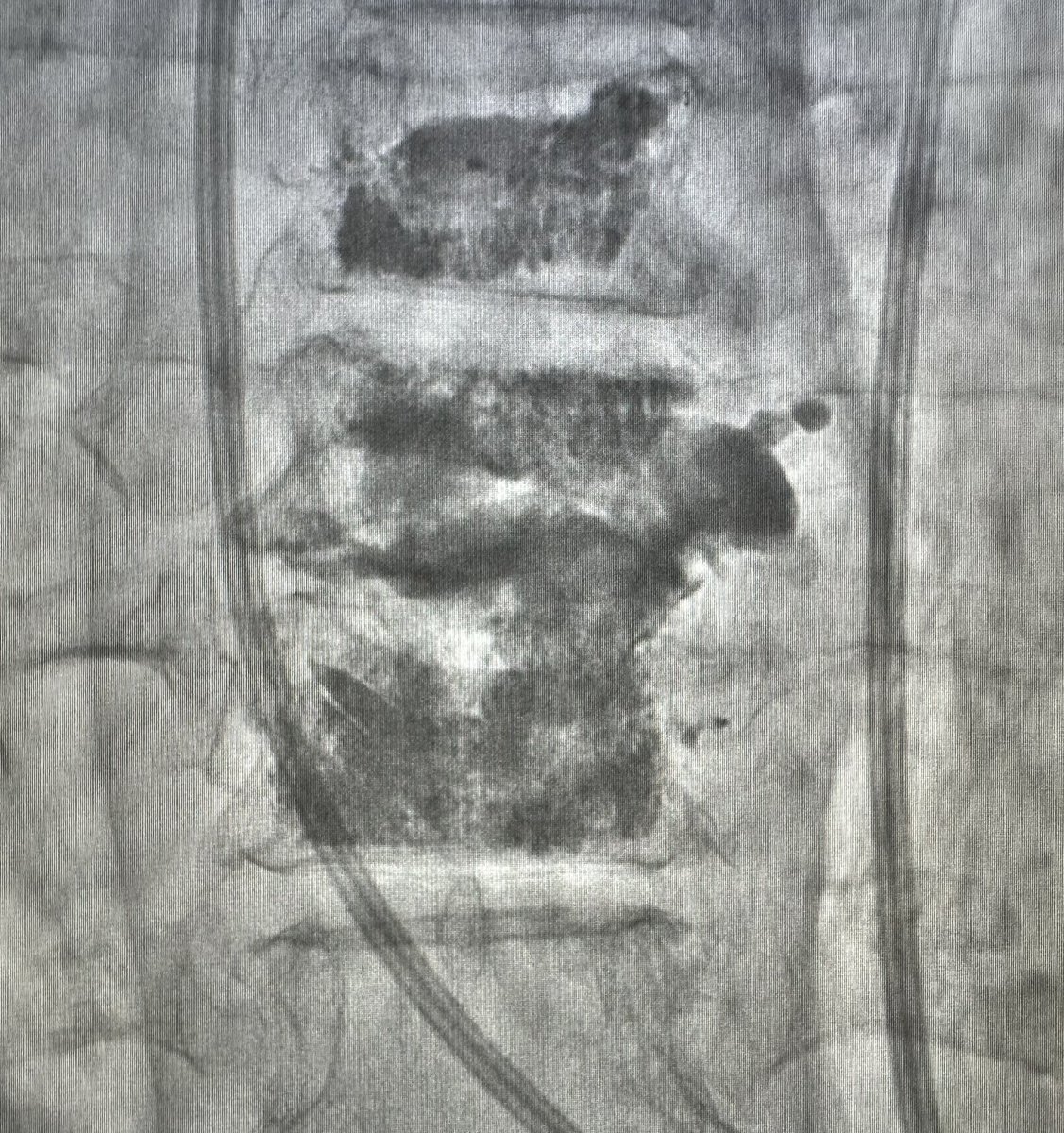
The main principle for treatment of hinge-fractures (DISH, ank spond) is stabilization, primarily from compressive forces. Cement from top of T9 to bottom of T10 accomplishes this.
Close follow-up to ensure stability and tx add'l fractures.
(3/) After initial cement from these accesses, the air filled fracture clefts are filled, but right side T10 is bare. Osteophyte blob = 👍🏼
Old accesses removed, new right transpedicular access with standard craniocaudal angulation. Moar curette. Curette = 🐐