
Lew Papendick
97 posts

The physician owned facilities were the same mixed bag of results as other facilities.
Both health outcomes and satisfaction.
And costs were also variable depending on the type of services offered.
My own view is widen who can own a facility but know that running a successful facility that is not putting brackets around the bottom line and getting the Star ratings right on outcomes and satisfaction is very complex work and requires integration of administrative and clinical roles to actually achieve those goals.
English

The ACA banned new physician-owned hospitals in 2010. Patient outcomes at POHs are better. Costs are lower. Satisfaction is higher. Now you know why they were banned.
English
@SalaryDr Cancel membership in AMA. Organize, fund, then lobby in IPA…Independent Physician Association.
English
Lew Papendick retweetledi
Rep. Greg Murphy is a physician. He sits on the Ways and Means Health Subcommittee, which sets Medicare physician payment rates.
The hospital industry gave him $54,650 in the 2024 cycle.
There is no allegation of wrongdoing here.
The contribution is legal.
The committee assignment is public.
The dollar amount is in the FEC filing.
What is worth noting is that the subcommittee responsible for physician payment contains a physician who received hospital industry money to sit on it.
The incentive structure produces rational actors.
Whether that is reassuring depends on which side of the fee schedule you are on.
@RepGregMurphy
@GOPDoctors
@WaysandMeansGOP

English
@BasedMikeLee @DataRepublican Go to work. Do the right thing.
English

The Senate GOP has exactly two options if it wants to avoid drifting into irrelevance and a stunning loss in November:
(1) Keep the filibuster and 60-vote cloture rule fully intact, but stand ready to overcome Senate Democrats’ unprecedented pattern of obstruction by aggressively enforcing the “talking filibuster”—a move that would require senators to work longer, harder hours and take fewer recesses, but lead to more thoughtful, careful deliberation in the legislative process,
OR
(2) Nuke the filibuster.
I strongly prefer the first option.
But we must choose either one or the other—because the status quo isn’t working and the resulting inertia isn’t just making it impossible to pursue a coherent agenda; it’s hurting the American people.
What’s your preference?
English
Lew Papendick retweetledi

Hello Senator Thune,
Let's expose what you're really doing with "reconciliation."
You announced it yesterday, eleven months after the House passed the SAVE America Act. You're not trying to pass this bill. You're trying to kill it in a way you can blame on process.
Here's how we know:
Reconciliation requires the Senate parliamentarian to rule that provisions are "budgetary." Citizenship verification is not budgetary. Photo ID mandates are not budgetary. The parliamentarian will gut the bill. Then you'll shrug and say "we tried." We see through you.
Meanwhile, you WON'T use the tools that actually work:
Rule XIX limits each senator to two speeches per legislative day. Keep the Senate in continuous session, file cloture daily, and the filibuster exhausts in ~12-20 days. You dismissed it as "complicated." Because if you tried and succeeded, you'd have to actually pass the bill.
Harry Reid nuked the filibuster in 2013 when he wanted results.
Mitch McConnell changed Senate rules THREE times and canceled the August recess.
Chuck Schumer used reconciliation within months on a 50-50 Senate.
You have 53 seats. You've changed nothing, canceled nothing, and waited eleven months.
Now let's talk donors:
• Goldman Sachs: $150K to you - top H-1B user
• Google: $75K - lobbies against E-Verify
• Meta: $72.5K - Zuckerberg's FWD[.]us pushes mass immigration
• Wells Fargo: $90K - banks undocumented immigrants
Same corporations sponsor Punchbowl News, where you sit for "Fly Out Days" which nobody watches except Congress staffers and K Street lobbyists who pays premium bucks for legislative intelligence. Their reporter then telegraphs to the audience the SAVE Act "will ultimately fail."
Corporate money flows to you AND to the outlet that frames your inaction as inevitable.
We see the loop.
You called grassroots anger a "paid influencer ecosystem." YOU are the paid influencer. You take the wrong side of a 80% issue because you are indistinguishable from a K Street mouthpiece, and an ineffective one to boot who won't bend the rules to get anything passed.
What we want:
1. Force a real talking filibuster.
2. Stop hiding behind process.
3. Pass the SAVE America Act.
YOU will become the reason that we will have our butts kicked in midterms. Not Candace Owens, not Nick Fuentes, not anyone else. You and you alone, and all because you want to make the 200 or so viewers of Punchbowl Fly Out Days happy. You're living in a K Street information bubble, addicted to the comforts and praises of lobbyists masquerading as journalists. You mistake the steak and martini dinners you get invited to as your own constituents.
You are not "moderate." The SAVE America Act has 98% support among Republicans. Name one other thing that has 98% support. You are an extreme minority who prides himself on being a calm leader, when in reality you are well in the running for the most ineffective Majority leader of all time.
Prove me wrong. Do the bare modicum of effort. Not symbolic. Actual effort. Cancel the recess. Get SAVE America Act passed.
English

It was an honor to testify in front of the @HouseCommerce subcommittee on health regarding healthcare affordability.
We discussed consolidation and the demise of independent physician practice.
My solutions include:
Repeal section 6001 of the ACA which banned physician owned hospitals
Reform Stark law
Implement site neutral payments
Reform 340B
Use FMAP to encourage states to be pro-competition (repeal CON, eliminate non competes)

English
Lew Papendick retweetledi

Lew Papendick retweetledi

Lew Papendick retweetledi
Here is an interesting thought experiment.
Name one other $5 trillion industry where the buyer commits to the transaction before knowing the price.
Not an estimate.
Not a range.
Not a “we’ll figure it out later.”
The actual price.
The number you will owe.
Before you agree to proceed.
You cannot.
Because in every other trillion-dollar market in human history, price discovery preceded the transaction.
Commodities have exchanges. Equities use public markets.
Energy has futures.
Real estate benchmarks comparables.
Healthcare did not skip price discovery because it is too complex.
Surgery is complicated.
So is refining oil.
So is pricing a mortgage-backed security.
Entrepreneurs found mechanisms for all of those.
Healthcare skipped price discovery because the intermediaries who sat between the buyer and the seller discovered that opacity was worth more than efficiency.
And then those intermediaries wrote the regulations that made the opacity structural.
Healthcare is not expensive.
Expensive implies a known price that is too high.
Healthcare is the one place where the price does not exist at the time of purchase.
This is an architecture problem and an opportunity.
Link in comments.

English
The AHA spent 15 years lobbying to make it illegal for physicians to own hospitals.
Not because physician-owned hospitals harm patients.
Because they reduce margins.
Every other claim is theater.
English

@DutchRojas Doctor should run hospitals. We put patients before profits. Executives by definition don’t know how to do that.
English
Jefferson Health’s top 28 executives received $47.3 million in compensation last year.
Jefferson’s charitable grants totaled $42.3 million.
The nonprofit’s management cost more than its charitable output.
I do not raise this as a complaint about executive compensation. Executives are expensive in most industries.
I raise it as a definitional question.
When the people running the charity cost more than the charity they run, the word “charity” is doing a great deal of work.
English
Lew Papendick retweetledi
A useful test for any regulatory framework:
Ask who lobbied for it.
The 2010 ACA ban on new physician-owned hospitals was lobbied by the American Hospital Association.
At the time, studies showed physician-owned hospitals had better patient outcomes and lower costs than hospital-owned facilities.
The AHA’s lobbying argument was not clinical.
It was market access.
The ban passed.
The outcomes data did not change.
The hospitals that lobbied against competition won.
The patients who would have been treated in those facilities represent an interesting counterfactual.
English
Lew Papendick retweetledi

A cool demonstration of physics.
The truck is moving forward at 80 km/h. The guy is catapulted in the opposite direction at 80 km/hr.
English
Lew Papendick retweetledi
You pay property taxes.
Jefferson Health does not.
$6.2 billion in tax-exempt real estate. $5.3 billion in tax-exempt bonds.
200 contract 340B pharmacies.
$47 million in executive compensation.
$201 million in operating losses.
And they just became the Official Health System Partner of the Philadelphia Eagles.
buff.ly/UJyWUs3 buff.ly/ybUSHD6

English
Lew Papendick retweetledi
Imagine whatever your job is. Now imagine someone who has never actually done that job designs the software you are required to use to do it.
Every single task now takes an extra 50 clicks. Things that could be handled with a quick verbal order now require logging in, navigating slow pop up windows, and clicking through reminders that add nothing to the outcome.
Now imagine your inbox fills with several hundred notifications a day. Most are useless. Buried somewhere in there might be the one message that actually matters.
When you want a simple improvement to the system, you are told it has to go through layers of committees and governance meetings, only to be denied. Yet when an administrator wants to add 20 more clicks or a new mandatory alert, there is no requirement to ask the doctors and nurses who actually use the software every day.
That is what is wrong.
English
@DrDiGiorgio 1. Repeal section 6001 ACA
2. Eliminate CON
3. Eliminate EPIC
4. Site neutral payment.
Română
Item 1: allow doctors to own hospitals
Item 2: eliminate Epic
Item 3: eliminate HIPAA
Item 4: eliminate metric reporting requirements
DrOzCMS@DrOzCMS
Join us for this year’s CMS Burden Reduction Conference on February 25th! We’re bringing together policymakers, healthcare providers, patients, and industry leaders to share innovative solutions to best address administrative burden across the healthcare ecosystem. Register online at go.cms.gov/4rgbnEm
English
Lew Papendick retweetledi
Dear Mr. Axelrod:
As you know, there are real, solvable structural issues in healthcare that deserve serious discussion.
For example:
• Repealing Section 6001 of the ACA
• Moving to site-neutral payments to eliminate site-of-service arbitrage
• Reducing reliance on centralized pricing mechanisms like the AMA RUC
• Encouraging transparent, market-based pricing models
• Reforming or eliminating outdated CON laws
None of these are abstract theories. They are policy choices.
CMS and Congress have the authority to address many of them, some by end of this week, and all of them by end of Q1-2026.
If the US government wants independent medicine, the lowest priced and most effective, small businesses to grow and patients to afford care, structural reform matters more than anecdotes.
Thank you,
Dutch
David Axelrod@davidaxelrod
Through family, I heard about a couple in WI who started a small business and were planning to expand. Now, with their ACA premiums TRIPLED due to congressional inaction, they've had to scrap plans to expand & grow. I'm sure that scenario is repeating itself all over the U.S.
English
Lew Papendick retweetledi
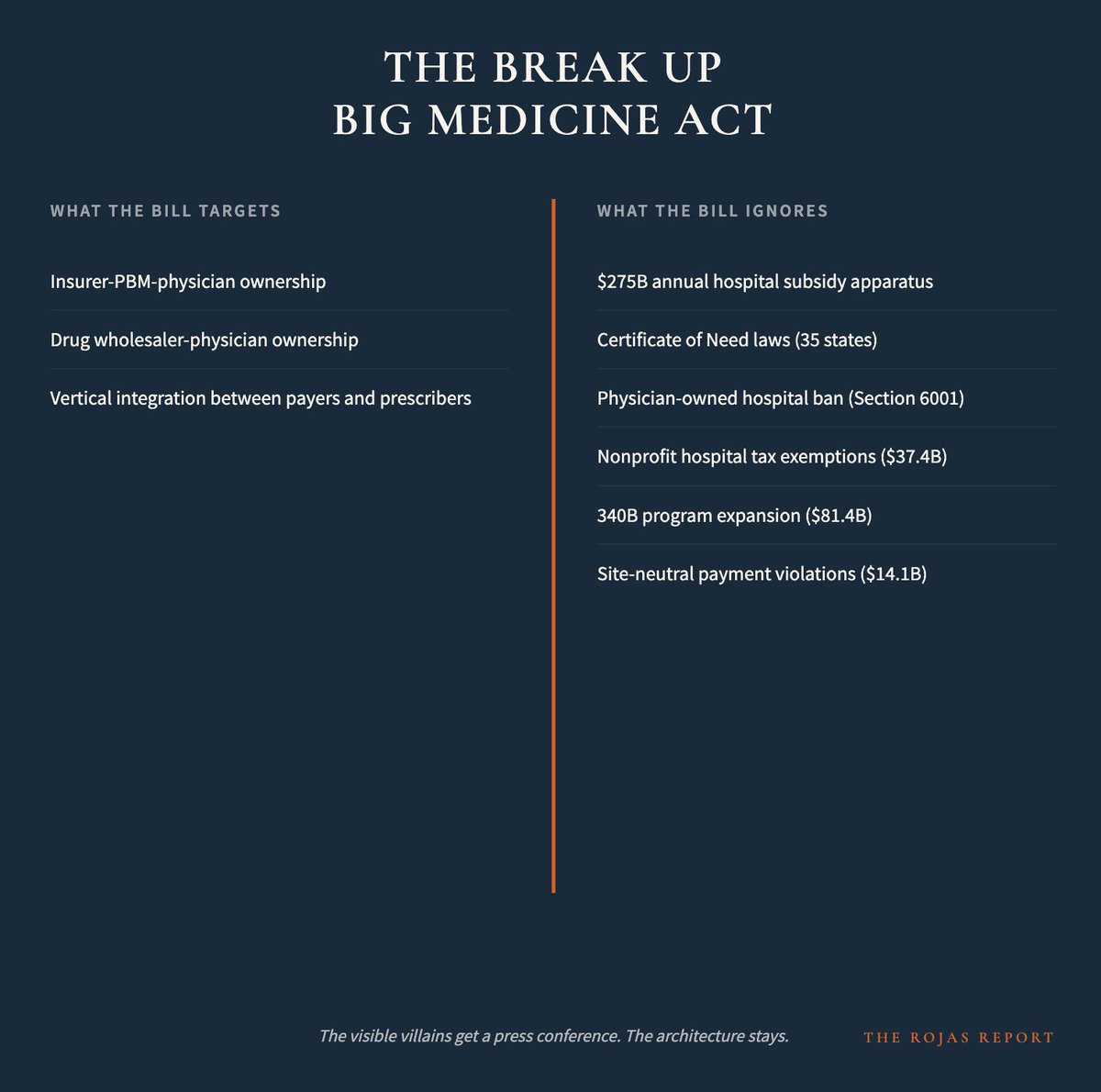
The real reform agenda is five items:
•Repeal the physician-owned hospital ban
•Eliminate Certificate of Need laws
•Enforce site-neutral payments
•Condition nonprofit tax exemptions on actual community benefit
•Separate insurer-PBM-physician conglomerates
This bill does one of five and calls it a revolution.
Do all of it, or admit the rest is theater.
buff.ly/k2aHceS
English
Lew Papendick retweetledi
$275 billion.
That’s how much the federal government takes from hard working Americans and hands to hospital systems every year in subsidies, tax breaks, and payment advantages.
Independent physicians receive $0 of it.
The Break Up Big Medicine Act touches $0 of it.
Not a coincidence.
Warren and Hawley love the American Hospital Association.
And where are the @GOPDoctors?
Nowhere.
English