
Lucas Massoth, M.D.
692 posts

Lucas Massoth, M.D.
@LucasMassoth
Hematopathologist & Surgical Pathologist | @MGHPathology @harvardmed trained | @UofOklahoma MD | @UArkansas Alum 🐗 | 🇺🇦
Katılım Mayıs 2020
666 Takip Edilen1.5K Takipçiler

Lucas Massoth, M.D. retweetledi

🔬YAP1::KMT2A‑rearranged sarcoma (with emphasis on diagnostic pitfalls)🔬
Rare fibroblastic sarcoma recently defined by YAP1::KMT2A fusion and a unique methylation profile, often mimicking sclerosing epithelioid fibrosarcoma (SEF), low‑grade fibromyxoid sarcoma (LGFMS), or even benign fibroblastic lesions.
Definition 📚
Soft tissue sarcoma characterized by YAP1–KMT2A/KMT2A–YAP1 fusions, SEF‑like/LGFMS‑like morphology, and an epigenetic cluster distinct from classic MUC4‑positive SEF and LGFMS.
Epidemiology 📊
Predominantly affects young to middle‑aged adults (median around 35–40 years, but a wide 9–90+ years range).
No clear sex predilection, with a slight male predominance in some series.
Sites 📍
Mainly arises in somatic soft tissues of trunk and extremities (deep or subcutaneous), including paraspinal regions, chest wall, axilla, and retroperitoneum.
Uncommon presentations include acral, suboccipital, and rare primary bone cases.
Pathogenesis 🧬
Driven by YAP1–KMT2A fusion, usually in a complex YAP1–KMT2A–YAP1 configuration, preserving the TEAD‑binding domain of YAP1 and the CXXC domain of KMT2A.
Unlike KMT2A‑rearranged leukemias, these tumors lack a strong HOXA signature, suggesting a distinct mechanism involving Hippo/YAP signaling and epigenetic remodeling.
Clinical Features 🩺
Presents as a slow‑growing mass, sometimes present for years, often becoming painful or clinically relevant only at later stages.
Initial pathology reports may label it as benign (fibromatosis, fibroma, “fibrous histiocytoma”) until recurrence or progression reveals malignant behavior.
Laboratory Diagnosis 🧪
No specific serum marker; diagnosis is histologic and molecular.
FISH for EWSR1/FUS is negative; FISH for KMT2A/YAP1 can be falsely negative, so broader DNA/RNA NGS panels or RNA‑seq are often required.
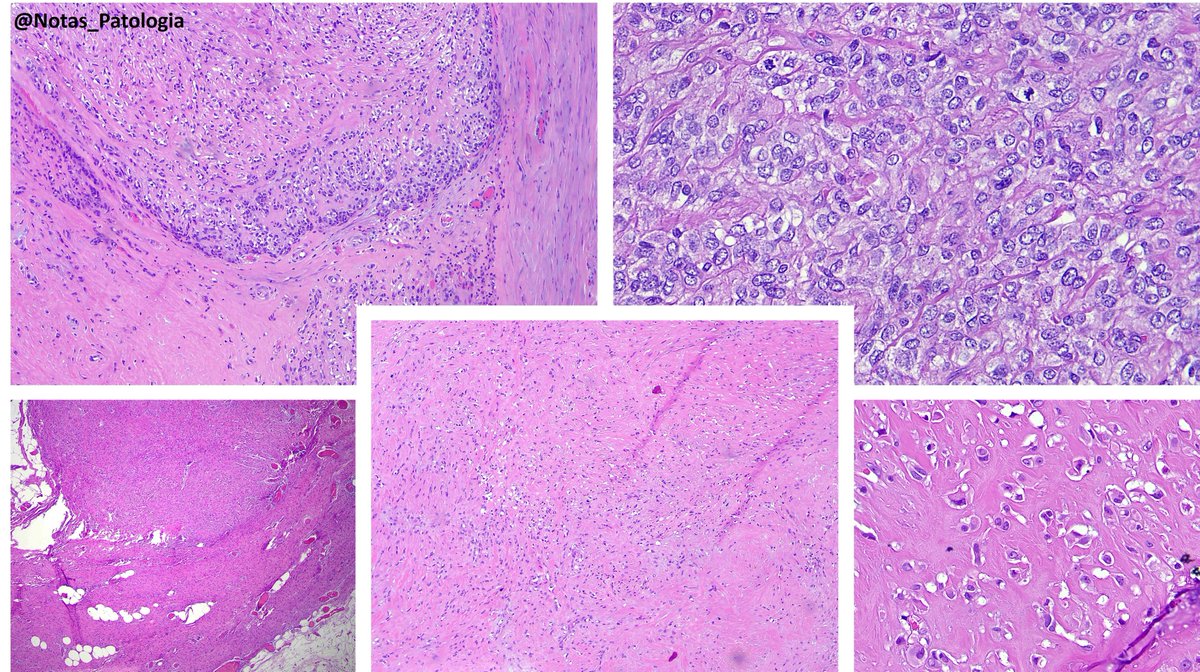
Histopathology 🔬
Architecture: grossly nodular tumors, but with infiltrative borders and “honeycomb” spread through subcutaneous fat and skeletal muscle.
Cytology: ovoid/epithelioid cells in cords, nests or solid sheets within dense collagenous stroma; mitotic activity usually low in hypocellular areas, higher in more solid/anaplastic foci.
Special patterns: perineurioma‑like areas (bland spindle cells in whorled/loose‑storiform pattern), fibroma‑like zones (very dense collagen with sparse cells), and foci of small round or rhabdoid cells in recurrences/metastases.
Additional findings: thin‑walled vessels (sometimes hemangiopericytoma‑like); typical absence of alternating fibromyxoid zones and classic collagen rosettes of LGFMS.
Immunohistochemistry 🧫
Positives:
EMA (diffuse or focal)
YAP1 (N‑ and C‑terminal)
Cyclin D1 in most cases
CD34 and SMA may be focally positive
Negatives:
MUC4 consistently negative (key point against classic SEF/LGFMS)
S100, SOX10, desmin, STAT6, most endothelial markers in typical cases
⚠️Notes:
Some tumors show strong ERG/CD31/D2‑40 and TFE3 expression, closely mimicking epithelioid hemangioendothelioma; in such cases, documentation of YAP1–KMT2A fusion and molecular clustering are crucial for correct classification.
Differential Diagnosis 🧠
Classic SEF – MUC4 strongly positive with EWSR1/FUS–CREB3L1 fusions, more frequent collagen rosettes and an overall more aggressive clinical course.
LGFMS – fibromyxoid pattern with arcades of vessels and collagen rosettes, MUC4 diffuse, FUS–CREB3L2/CREB3L1 fusions.
Perineurioma/DFSP – honeycomb infiltration and CD34 expression may overlap, but they lack SEF‑like morphology and YAP1–KMT2A fusion.
Epithelioid hemangioendothelioma – blister cells and endothelial markers; typical EHE harbors WWTR1/YAP1–TFE3 fusions and falls into a different molecular cluster.
Fibromatosis/scar – fibroma‑like areas may mislead; subtle atypia, transition to more cellular SEF‑like zones, and EMA/cyclin D1 expression favor sarcoma.
Prognosis 📈
Intermediate prognosis between LGFMS and classic SEF: local recurrence in roughly 20–30% and metastases in about 50% of patients with follow‑up, mainly to lungs/pleura.
Overall survival is worse than LGFMS but better than classic SEF; robust histologic or molecular risk stratifiers within this group are not yet well defined.
Treatment 💉
Mainstay is wide surgical excision with negative margins, often combined with adjuvant radiotherapy for deep‑seated or margin‑positive lesions.
Evidence for systemic chemotherapy is limited; extrapolation from SEF suggests modest responses to conventional sarcoma regimens, and no validated targeted therapies are currently established for this fusion.
Take-Home Messages @Notas_Patologia ✅
📌Consider YAP1::KMT2A‑rearranged sarcoma in SEF‑like/LGFMS‑like tumors that are MUC4‑negative.
MUC4 negativity + EMA/cyclin D1 positivity and a YAP1–KMT2A fusion define the diagnosis.
📌FISH for KMT2A/YAP1 may be falsely negative – broader NGS or RNA‑seq is often needed.
📌DNA methylation profiling shows a distinct cluster, separate from SEF and LGFMS.
📌Clinically, this is a malignant sarcoma with a real risk of lung metastasis, even when histology appears deceptively bland.
Selected References 📖
Warmke LM et al. YAP1::KMT2A‑rearranged sarcomas harbor a unique methylation profile and are distinct from sclerosing epithelioid fibrosarcoma and low‑grade fibromyxoid sarcoma. Virchows Arch, 2024.
Massoth LR et al. Pan‑sarcoma genomic analysis of KMT2A rearrangements reveals distinct subtypes defined by YAP1–KMT2A–YAP1 and VIM–KMT2A fusions. Modern Pathology, 2020.
Puls F et al. Recurrent fusions between YAP1 and KMT2A in morphologically distinct neoplasms within the spectrum of low‑grade fibromyxoid sarcoma and sclerosing epithelioid fibrosarcoma. American Journal of Surgical Pathology, 2020.
Agarwal A et al. YAP1–KMT2A fusion‑positive sarcoma: an emerging soft tissue tumor entity with morphological features resembling sclerosing epithelioid fibrosarcoma. Indian Journal of Pathology and Microbiology, 2024.
⚠️Disclaimer⚠️
“This text is an educational summary for healthcare professionals and students. It does not replace full pathology reports, local guidelines, or individualized clinical decision-making.”
Hashtags:
#MedicalEducation #NotasDePatologia #SoftTissuePathology #Sarcoma #PathTwitter
🖋️ Case and slide coloration courtesy of Dr. Alexandre Carneiro (@AmcarneiroMD), as part of an academic partnership project.
English
Lucas Massoth, M.D. retweetledi

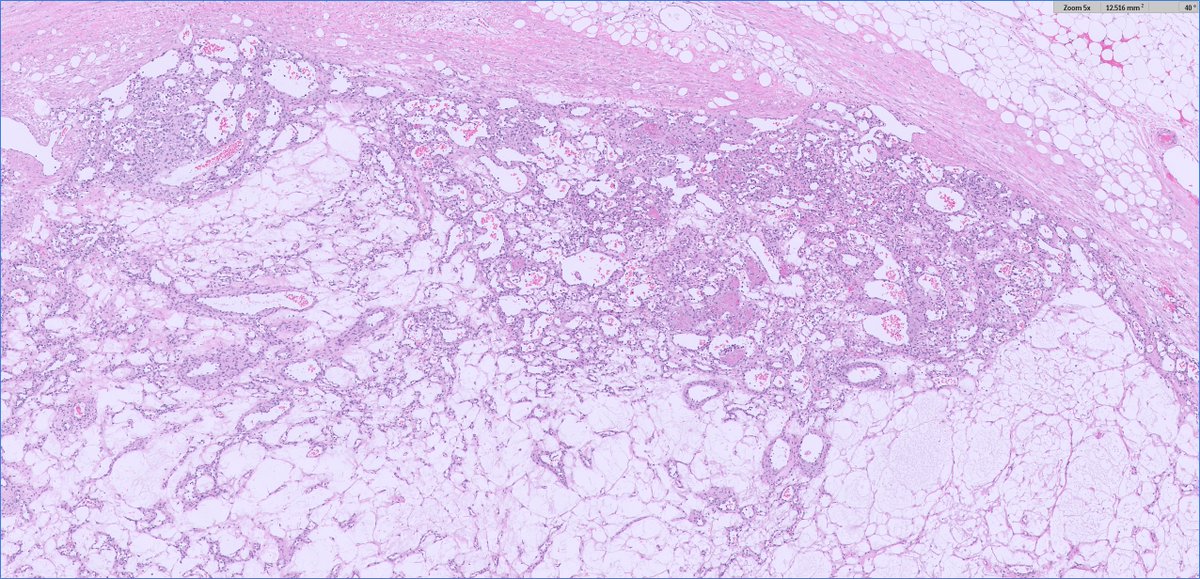
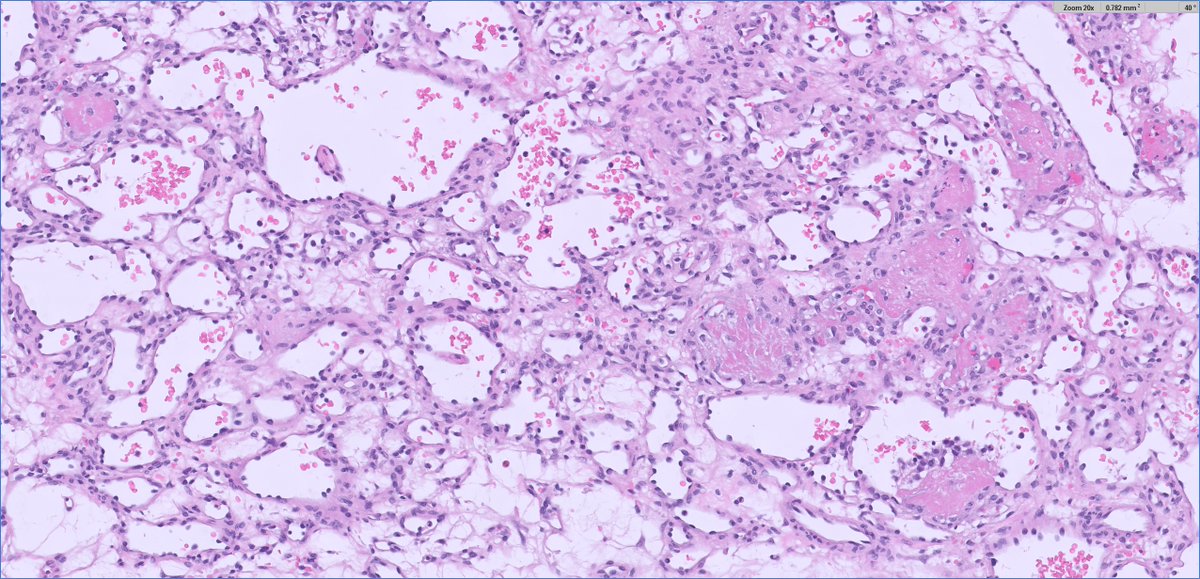
#GUpath🧩time!
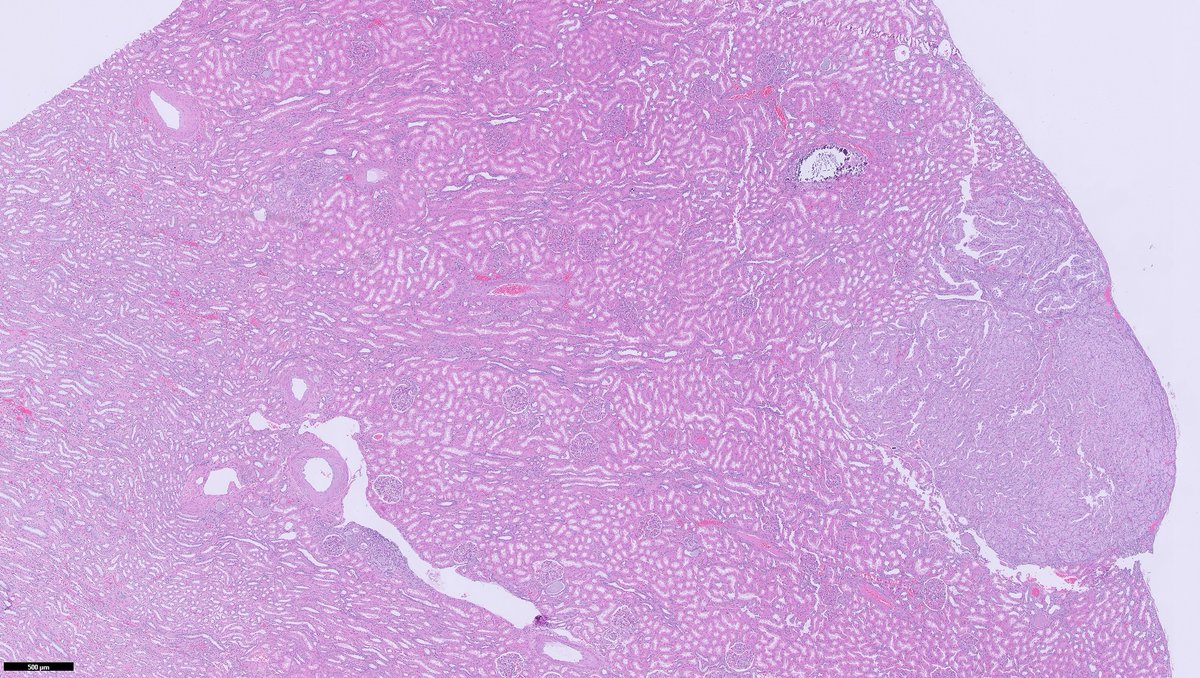
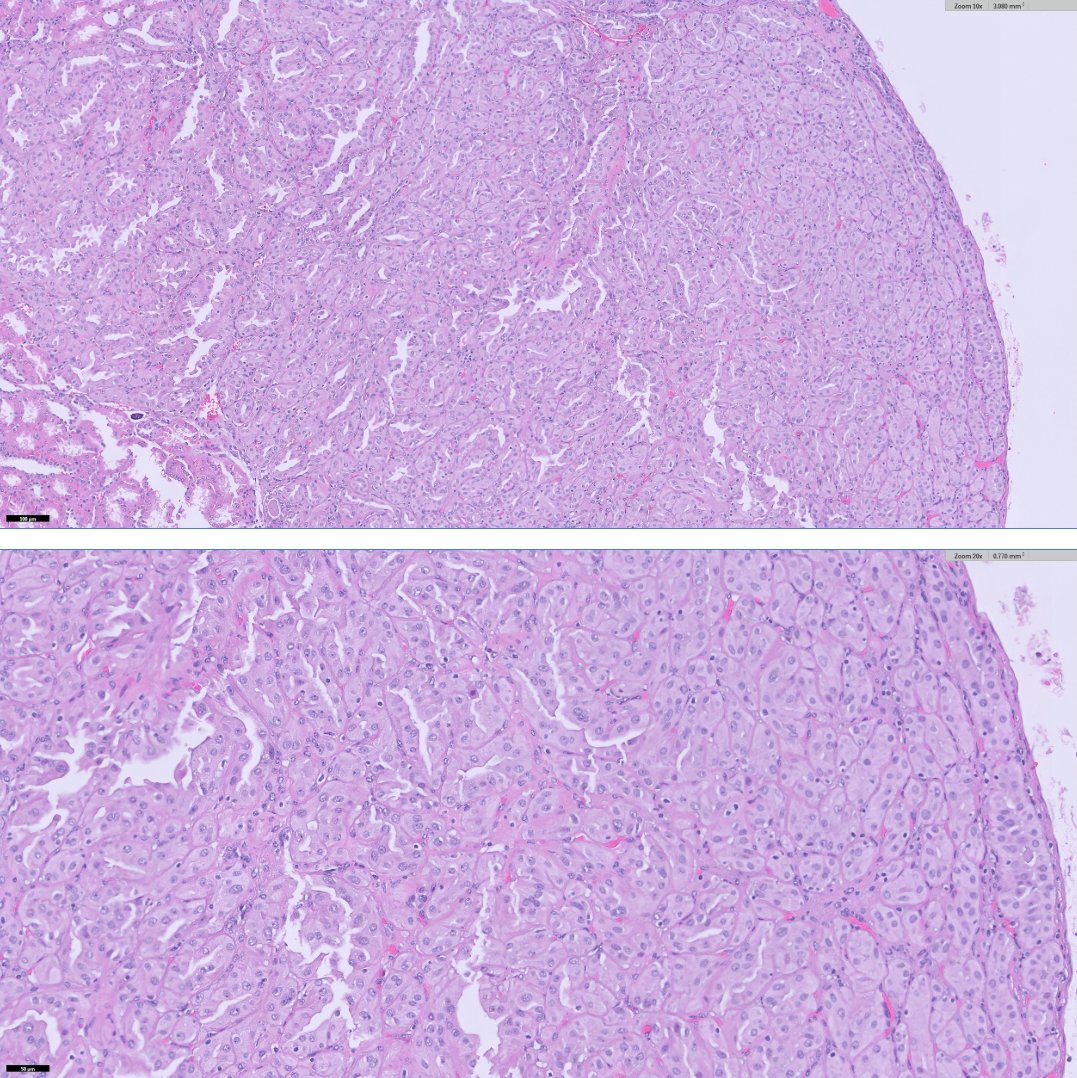
40ish F undergoes partial nephrectomy for larger epithelioid AML (not shown here)
in background kidney, 3mm nodule identified (👇🏽👇🏽)
I'll let folks🤔& list out their TOP 5 DDx in any order, and not comment
(I'll do one single reply to my original post later)


English
Lucas Massoth, M.D. retweetledi


English
Lucas Massoth, M.D. retweetledi


Lucas Massoth, M.D. retweetledi


English
@dgbrackett @smlungpathguy Thank you! We are up to two now, not sure we can handle anymore 🤣 I will shoot you a DM
English

@LucasMassoth @smlungpathguy Hi Lucas! I couldn't help but notice the small child in your profile photo - congrats! 🥰So much time has passed! Hope you guys have been well.
English
@smlungpathguy BAL of my personal favorite—can be a little tough to distinguish from leishmaniasis morphologically, but living in the Mississippi River valley helps immensely! #histoplasmosis #PathTwitter

Sanjay Mukhopadhyay@smlungpathguy
Diagnose by morphology (on surgical pathology) or give a differential diagnosis and defer to cultures? See the answer here: journals.sagepub.com/doi/10.1177/10…
English
@DrMarkOng @DanGrahamMD I too thought this was most likely to be a vascular malignancy based on h&e but the negative ERG is stumping me. I’d go more broad - add on cd34, HHV8, CD45, S100, INI, synaptophisin, and maybe a MOC31. Hopefully something hits before the lab runs out of stains!
English
@DanGrahamMD @LucasMassoth Lots of entrapped red blood cells. Angiosarcoma based on CD31?!
English

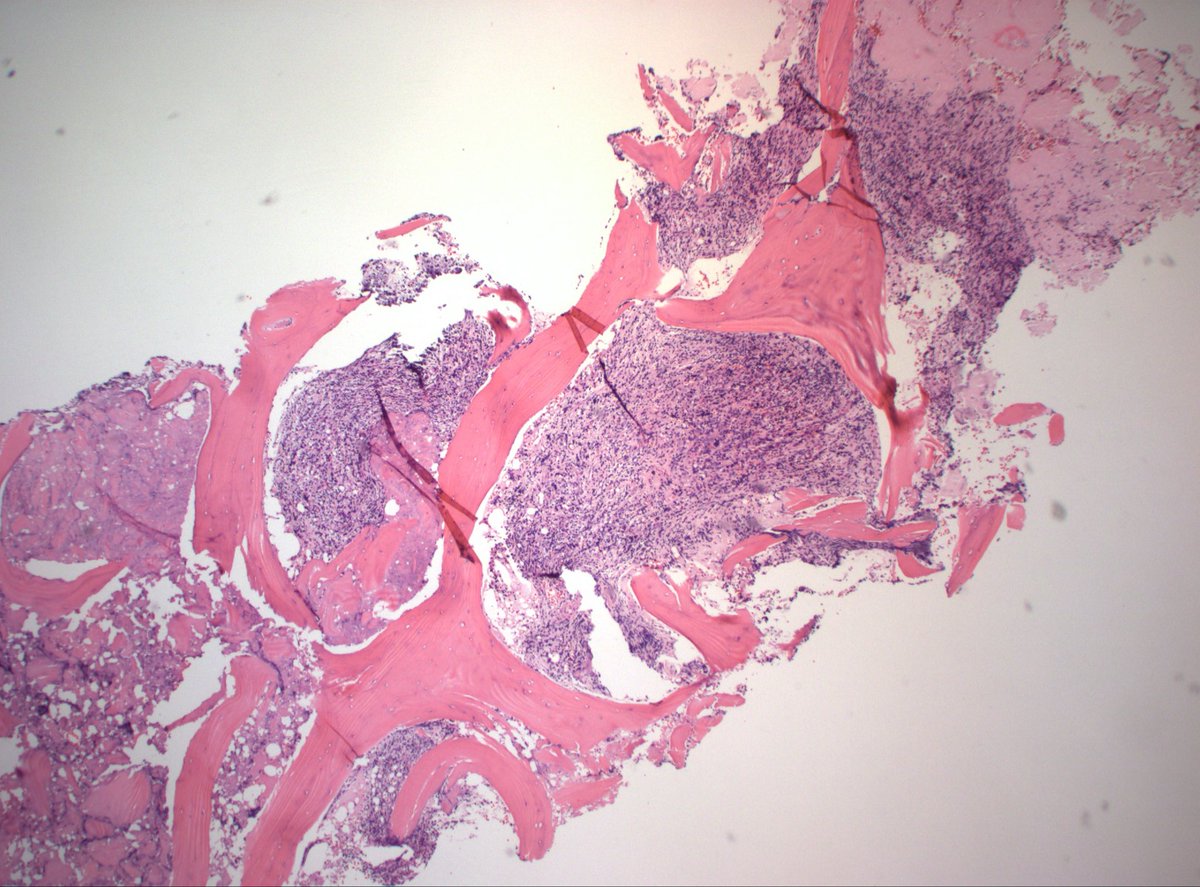
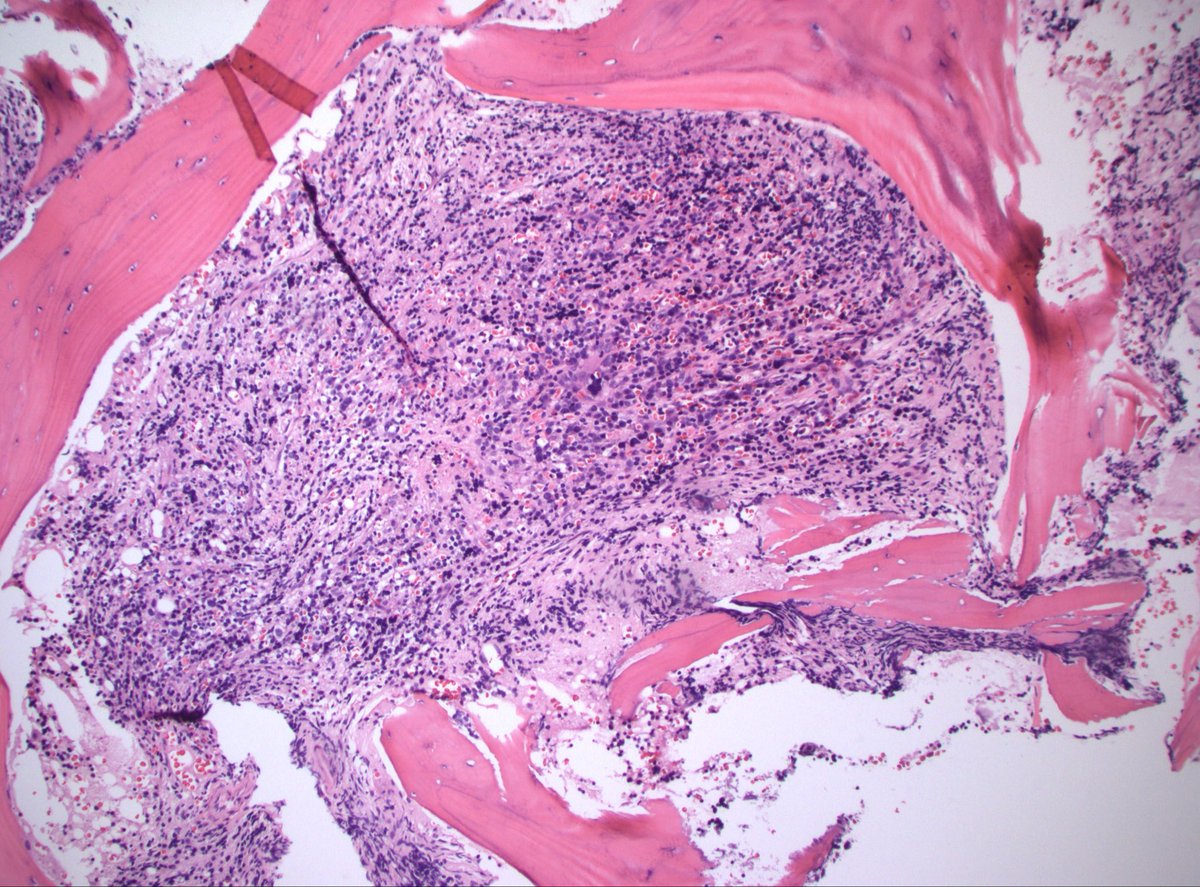
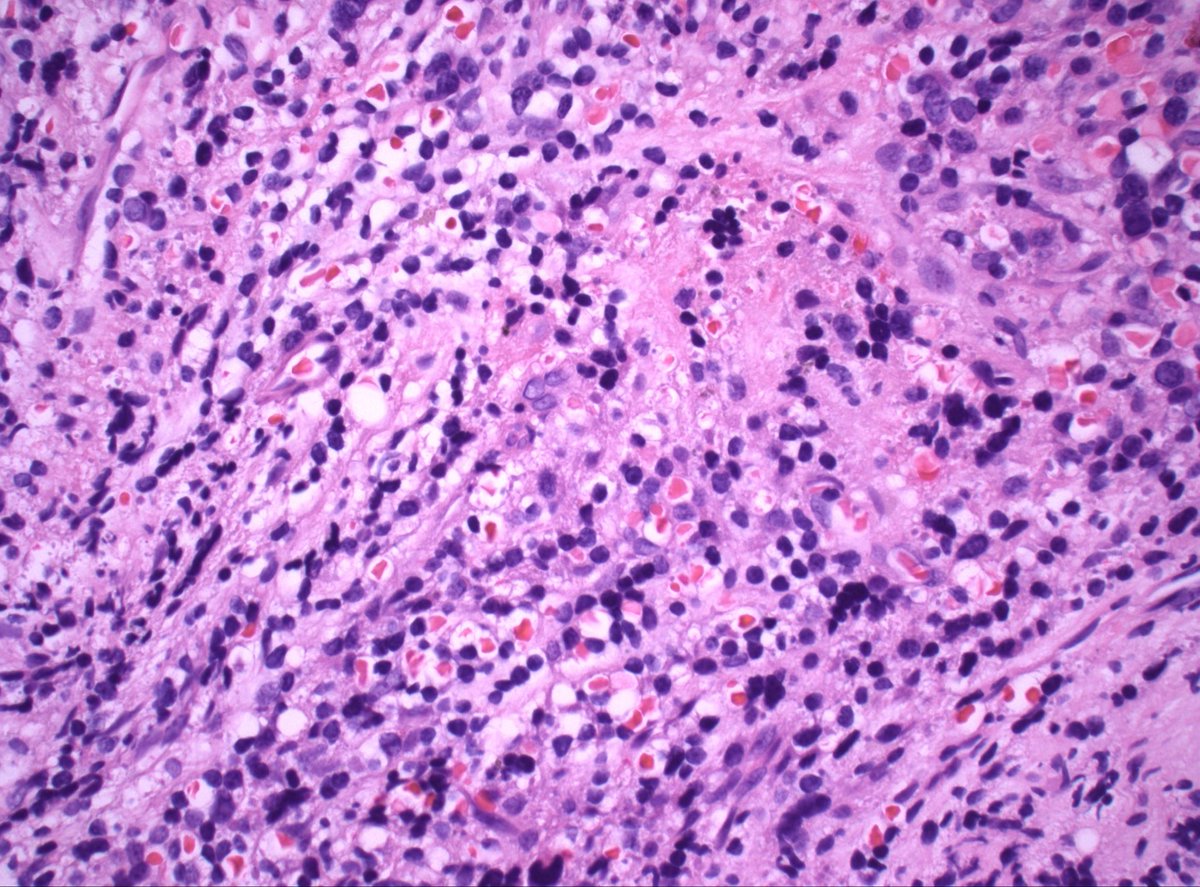
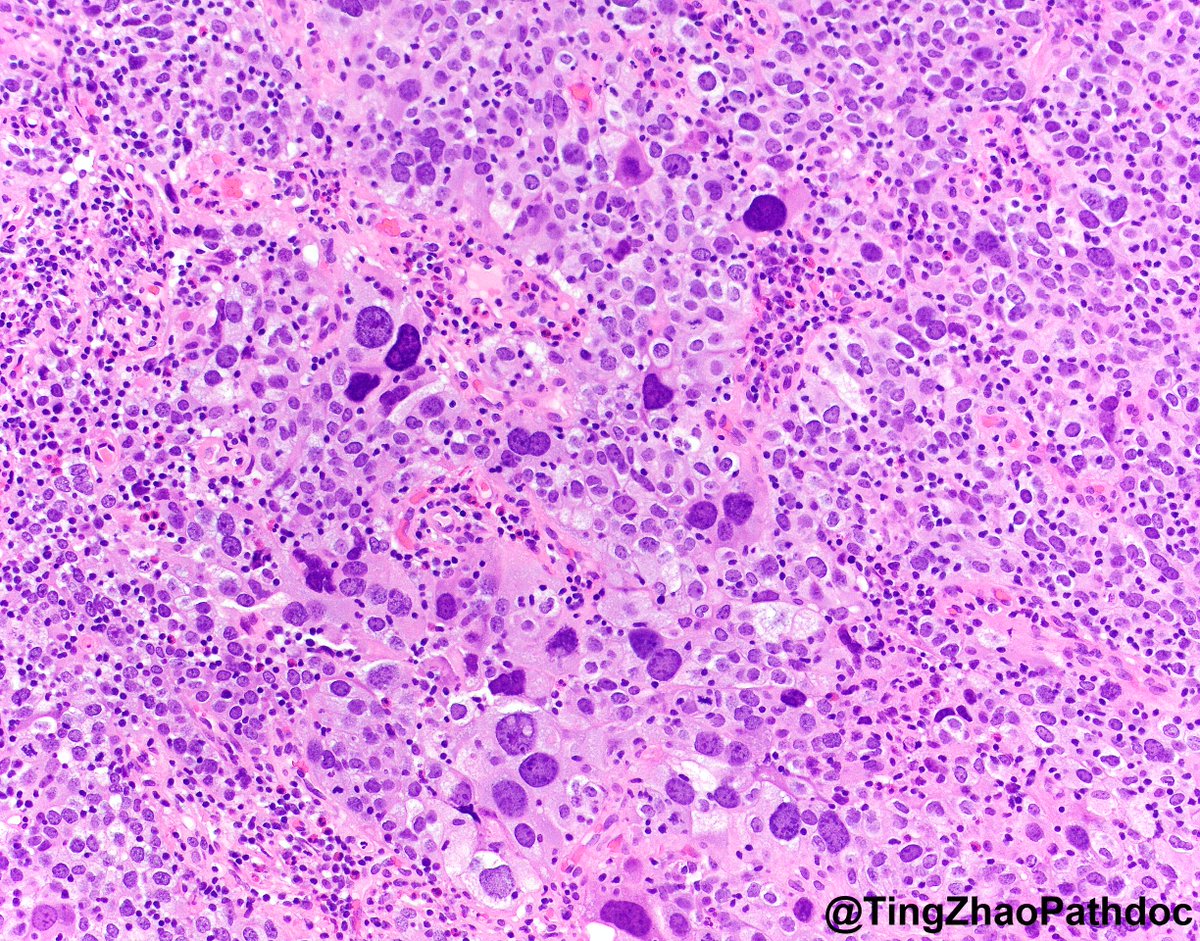
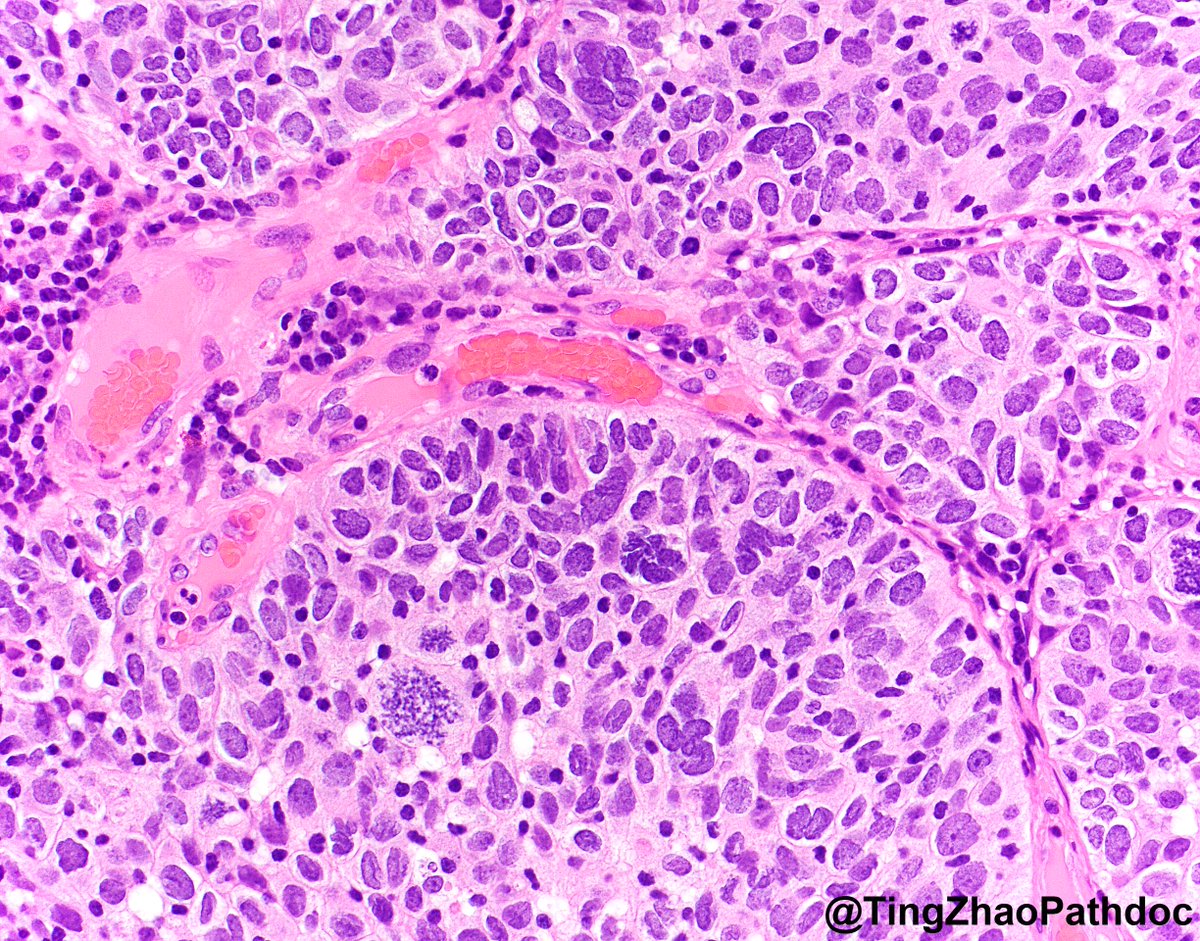
70s M h/o prostate cancer. Multiple bone lesions, this one from iliac. Dx/workup?
#PathX #PathTwitter
English
Lucas Massoth, M.D. retweetledi

100% agree. The power of clinical context should not be ignored. The decision of how much relative weight should be placed on clinical setting vs pathologic findings is tricky, and requires judgement and skill
Lucas Massoth, M.D.@LucasMassoth
@smlungpathguy BAL of my personal favorite—can be a little tough to distinguish from leishmaniasis morphologically, but living in the Mississippi River valley helps immensely! #histoplasmosis #PathTwitter
English
English
60s F, bladder transurethral resection. What is your diagnosis?
#PathTwitter
@MGBpathology @MGHPathology
English
Diagnose by morphology (on surgical pathology) or give a differential diagnosis and defer to cultures?
See the answer here:
journals.sagepub.com/doi/10.1177/10…

English
Lucas Massoth, M.D. retweetledi

Lucas Massoth, M.D. retweetledi

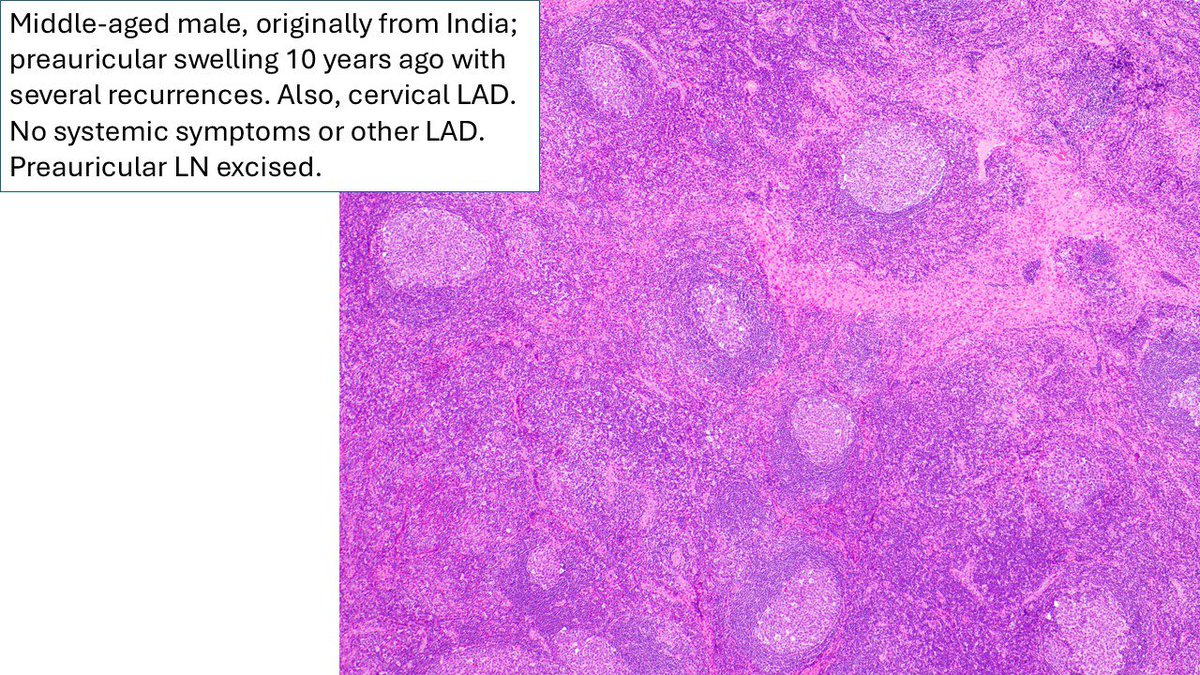
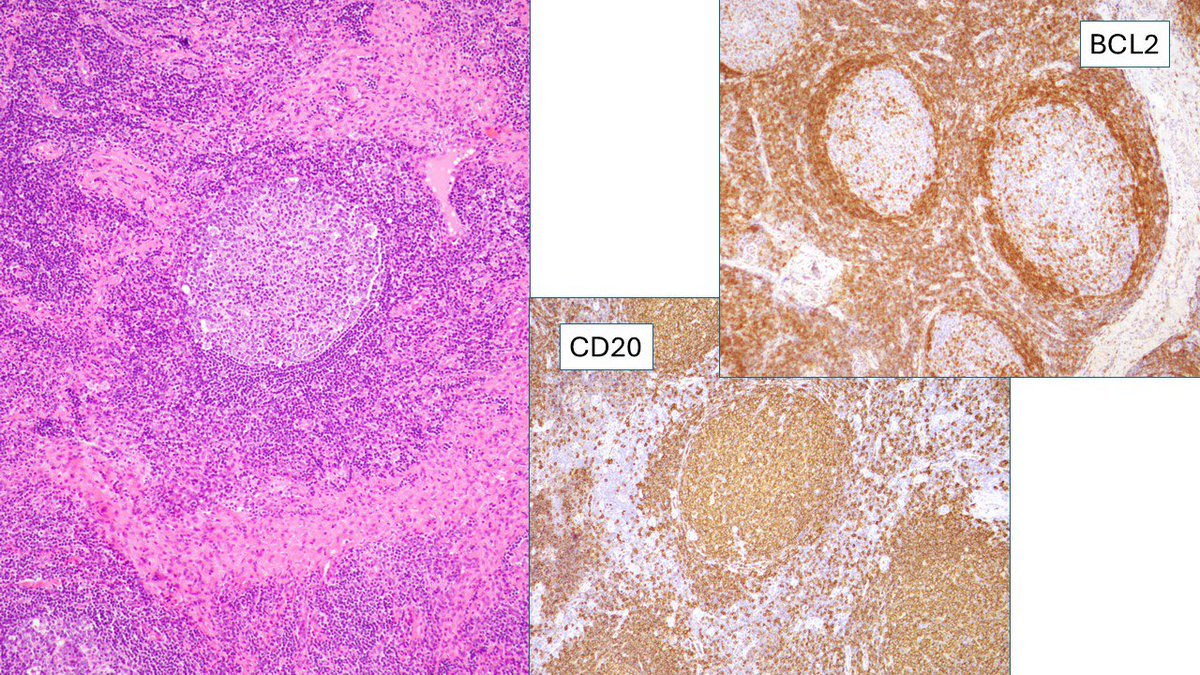
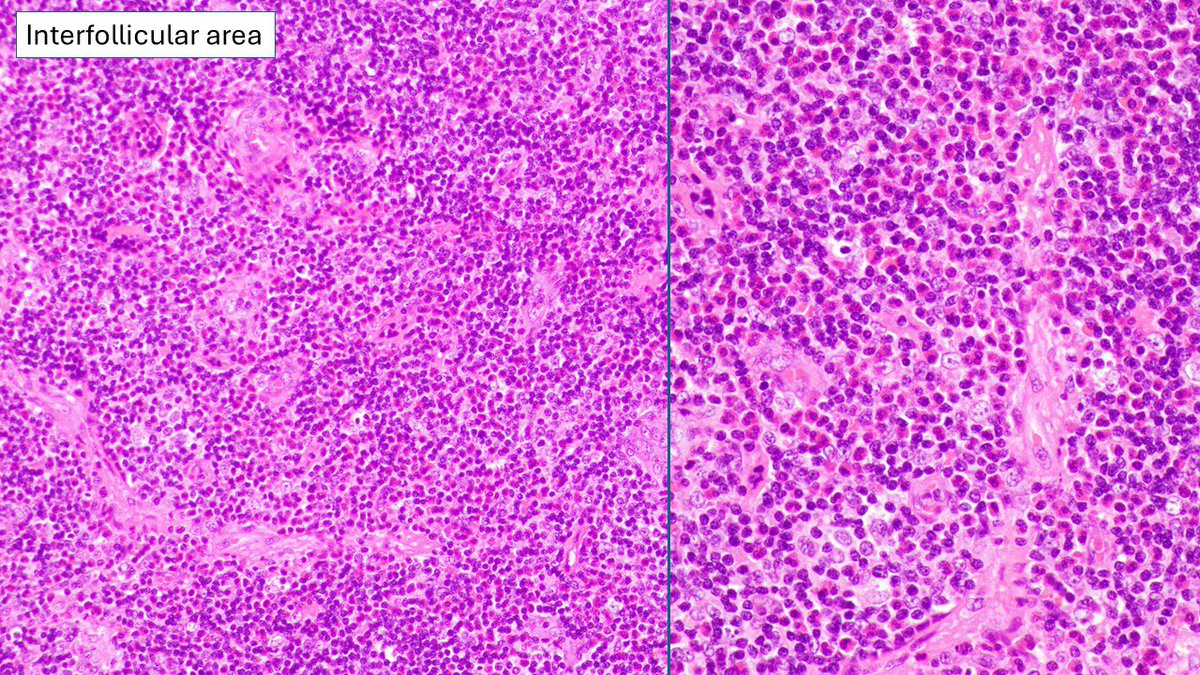
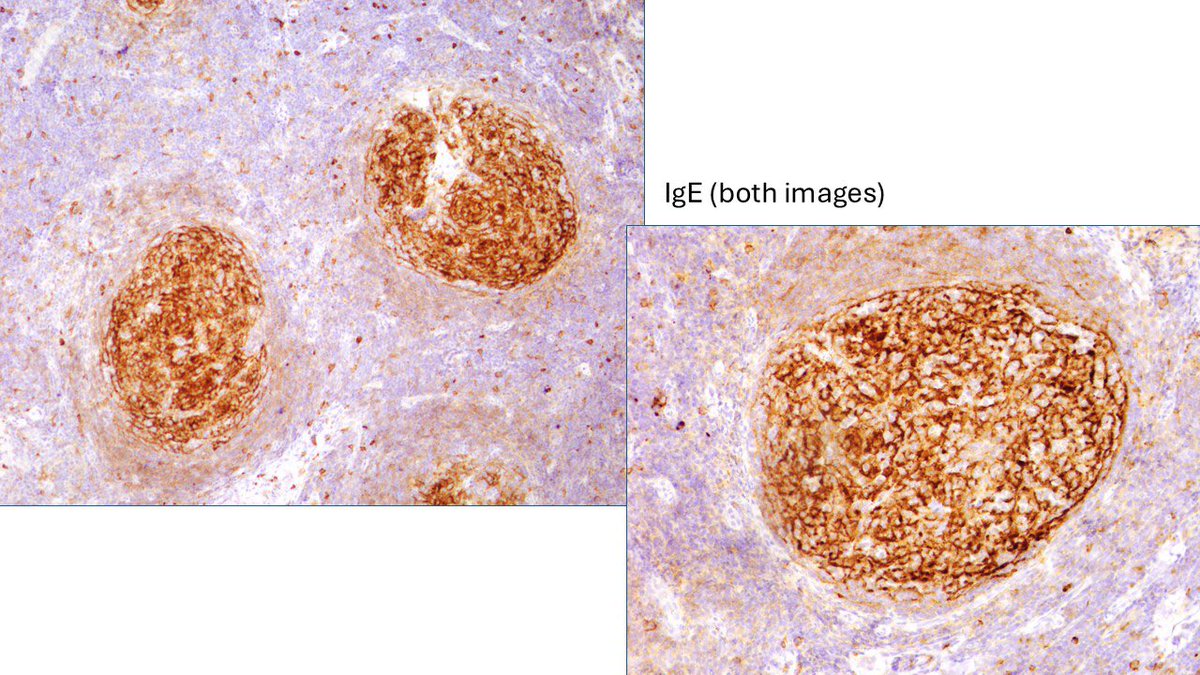
I called this reactive lymphoid hyperplasia consistent with Kimura’s disease. Apologies also for the typo: pre-articular should have been preauricular. Damn AutoCorrect. #Kimuradisease #Eosinophils #IGE.
Judith Ferry@judith_ferry
Pathologists! What do you make of this enlarged pre-articular lymph node in adult male originally from India? Otherwise, asymptomatic, no enlarged nodes away from head and neck. #HemePath #Lymphadenopathy #lymphnode
Cambridge, MA 🇺🇸 English
Lucas Massoth, M.D. retweetledi
Pathologists! What do you make of this enlarged pre-articular lymph node in adult male originally from India? Otherwise, asymptomatic, no enlarged nodes away from head and neck. #HemePath #Lymphadenopathy #lymphnode
Boston, MA 🇺🇸 English
Deutsch

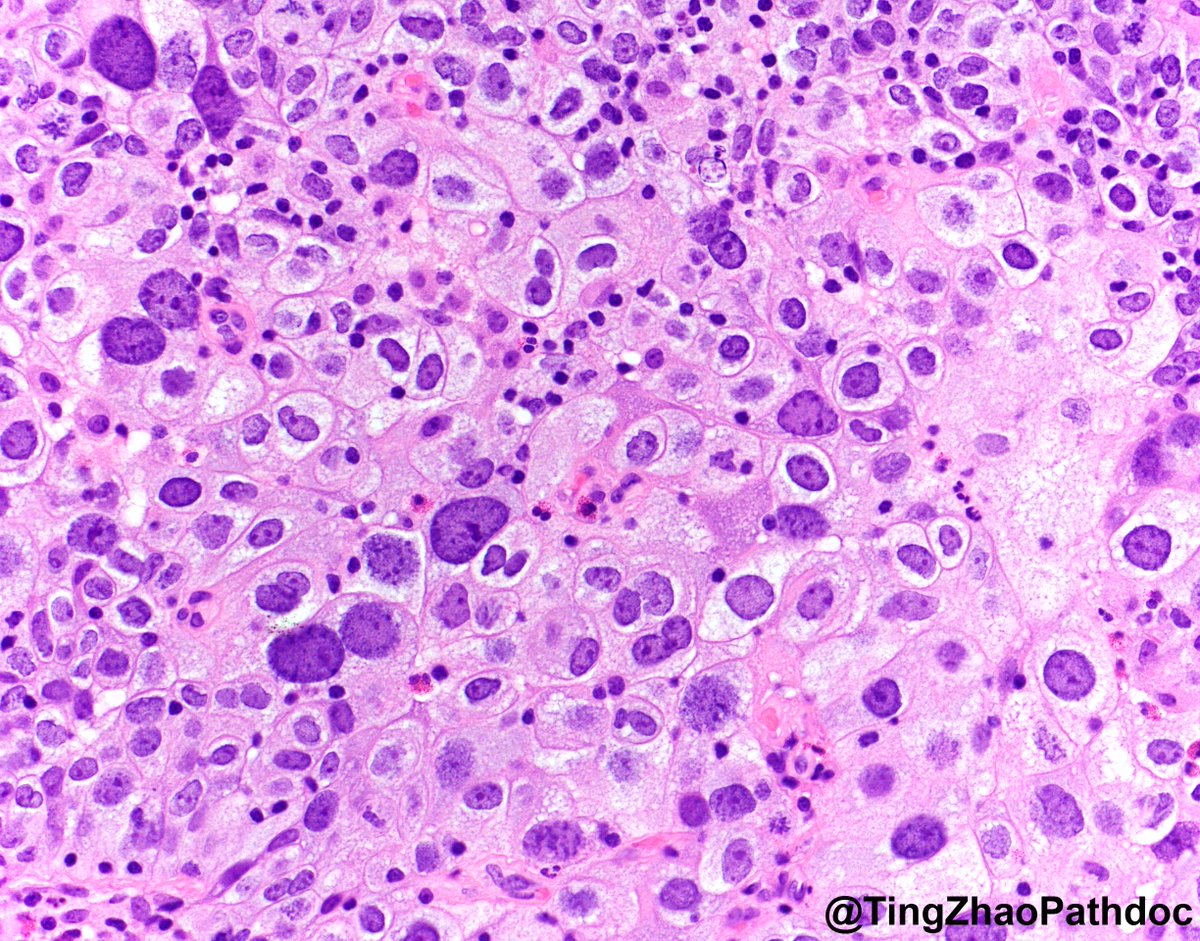
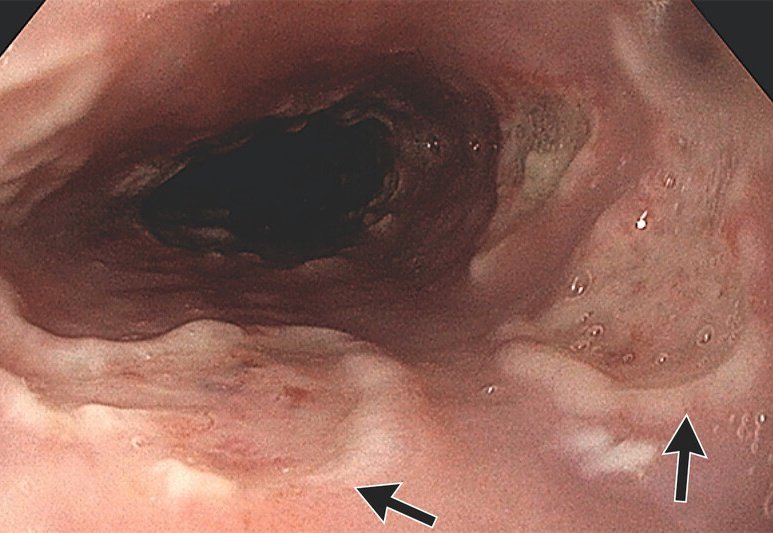
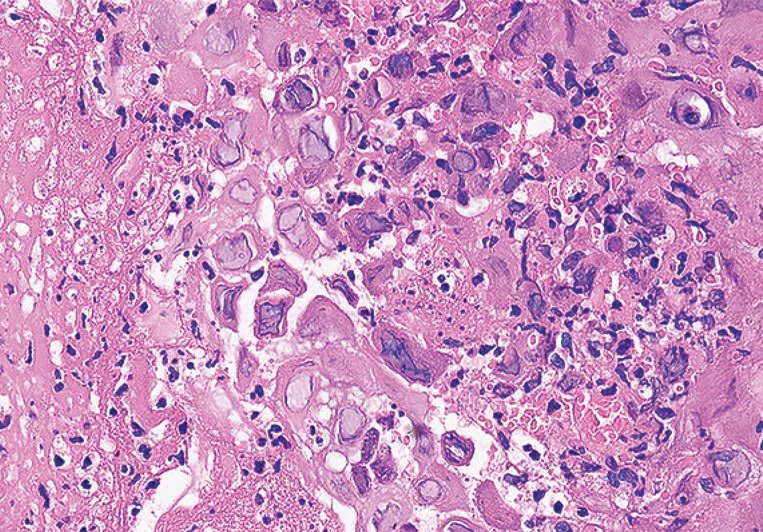
56, female, presents with difficulty swallowing 140 days after allogeneic transplant for AML 😭
GI scopes her, sees 👇🏽
Path sees 👇🏽
What's going on?
Management?
English
Lucas Massoth, M.D. retweetledi

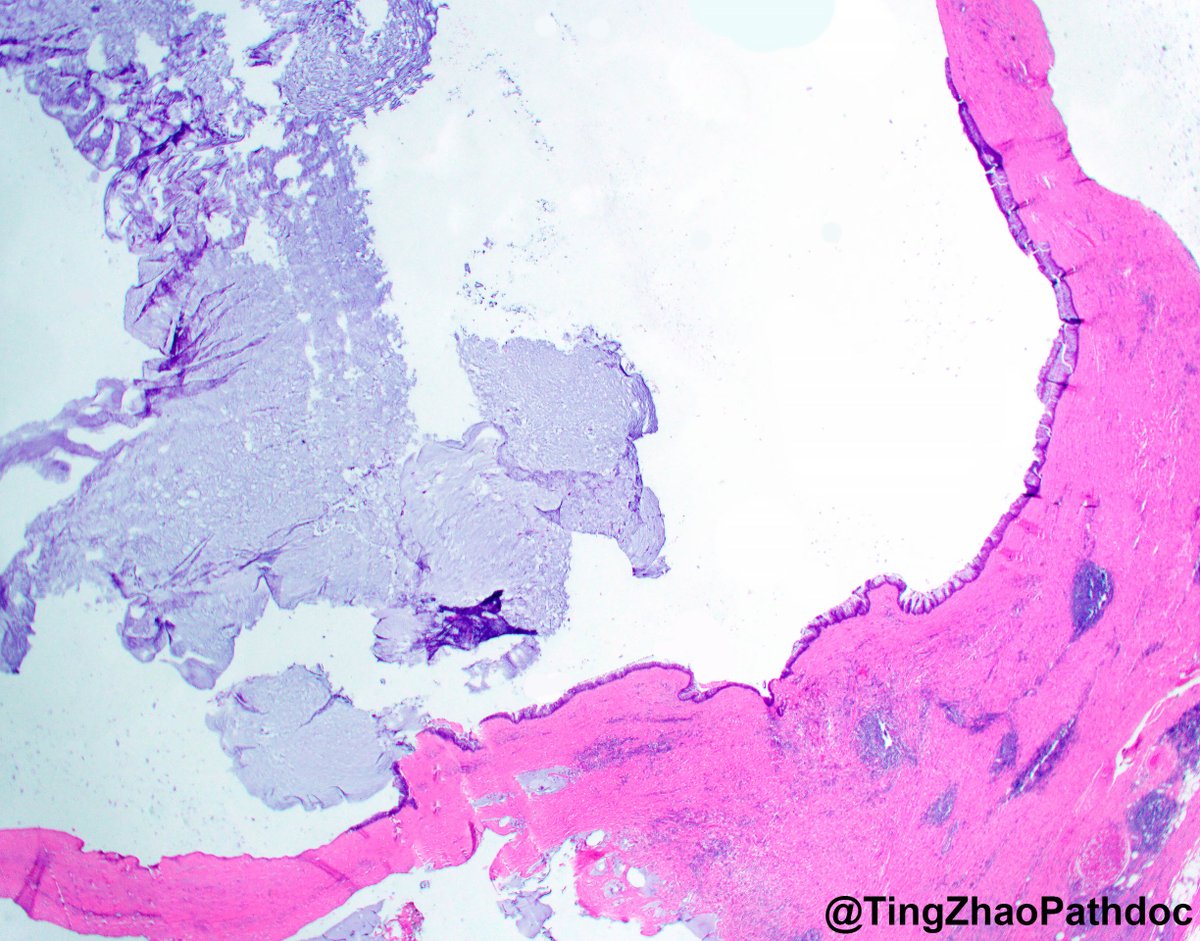
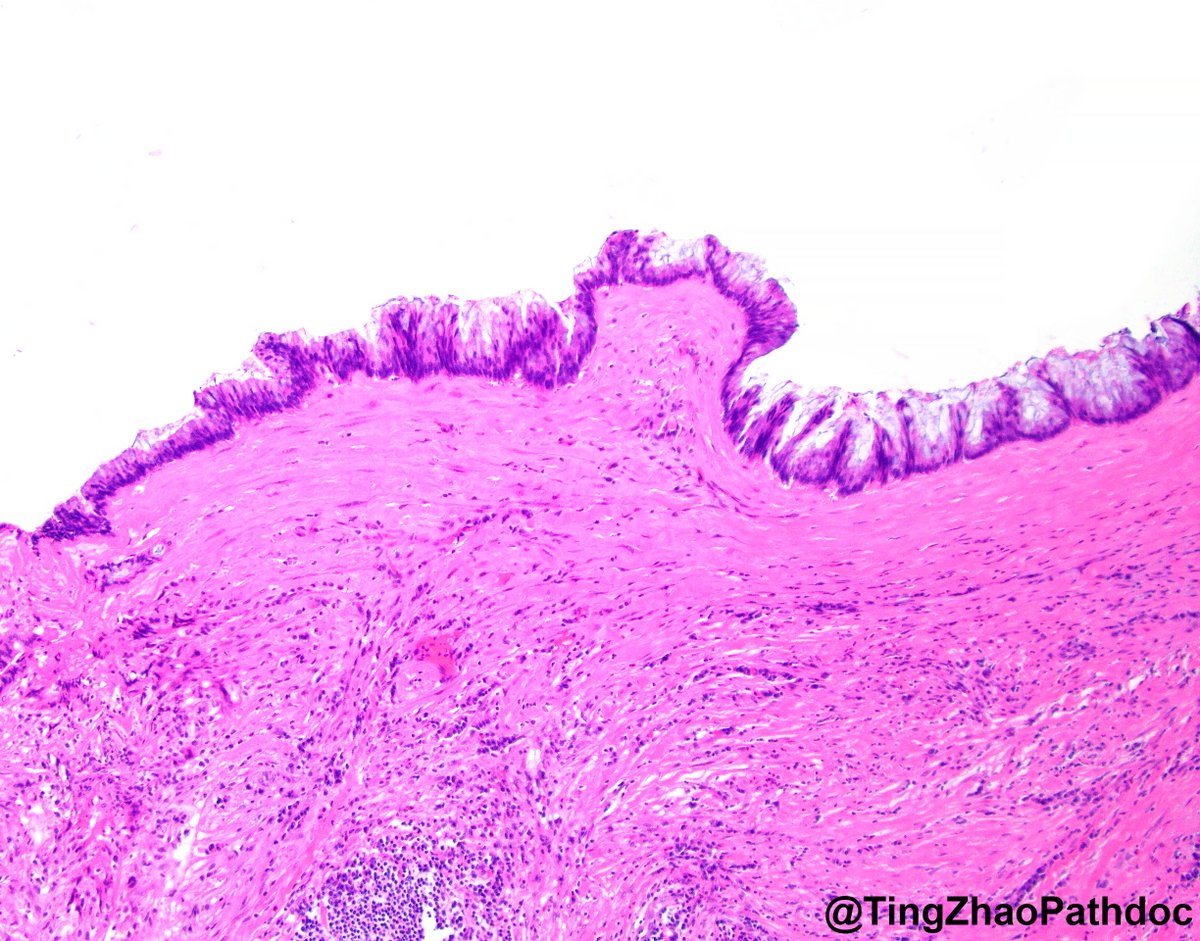
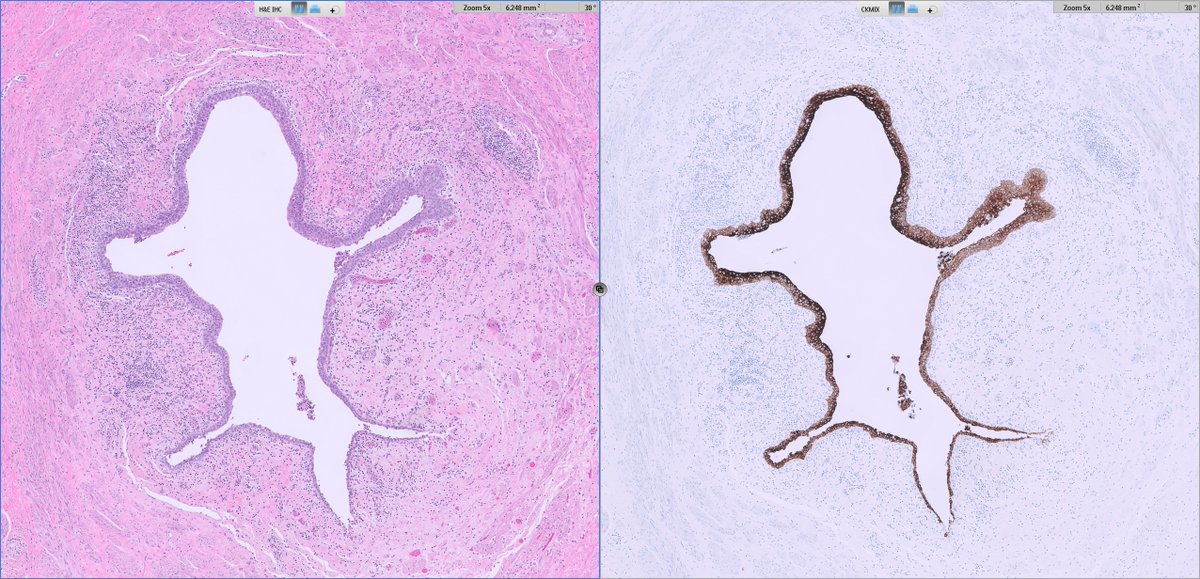
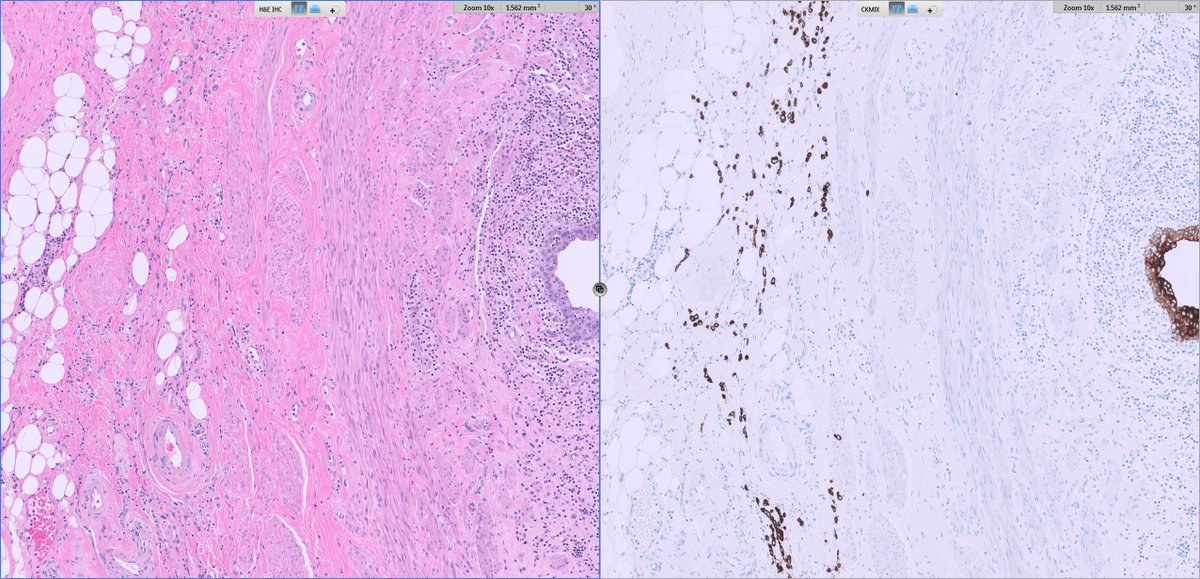
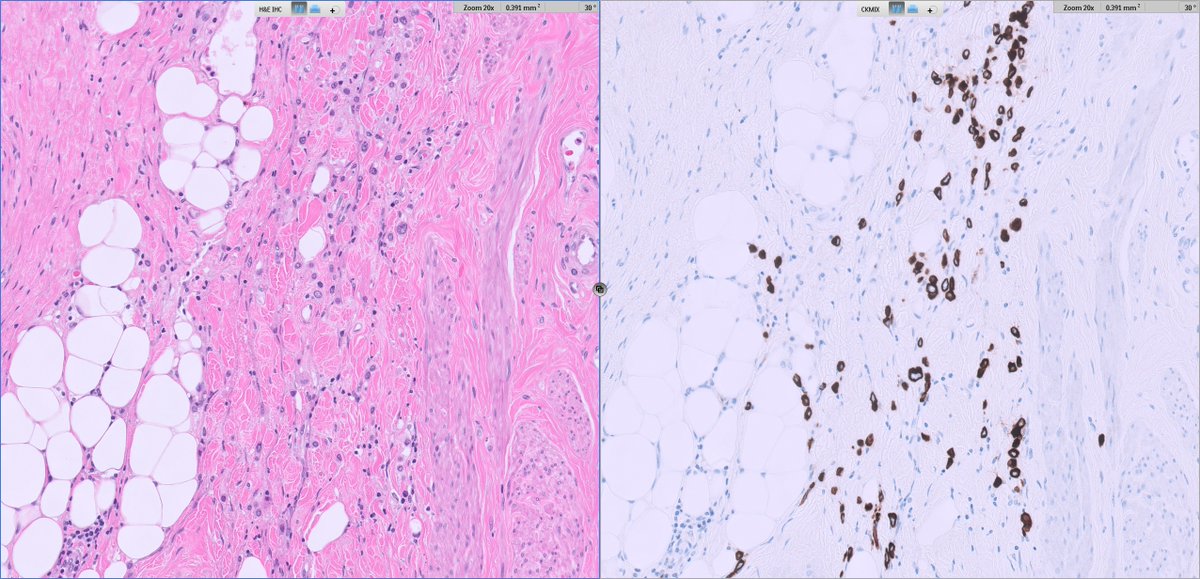
From the inky depths of your differentials, a mysterious tumor arises 🎃👻
Which breast lesion haunts your microscope? 🦇🦇🦇🧛♂️🦇🦇🦇
Cast your vote in the comments—if you dare. 🧟♂️
Answer revealed Monday. 🕸️
#PathX #PathTwitter #breastpath

English
Lucas Massoth, M.D. retweetledi

English
Lucas Massoth, M.D. retweetledi
Love to learn pathology? Come to Vegas and learn stuff you can really use in your practice!
Faculty include: @Williamson_SR @RazaHoda @smlungpathguy , Karuna Garg and Jacob Sweeney
Register here: clevelandclinicmeded.com/live/courses/p…
English