Sabitlenmiş Tweet

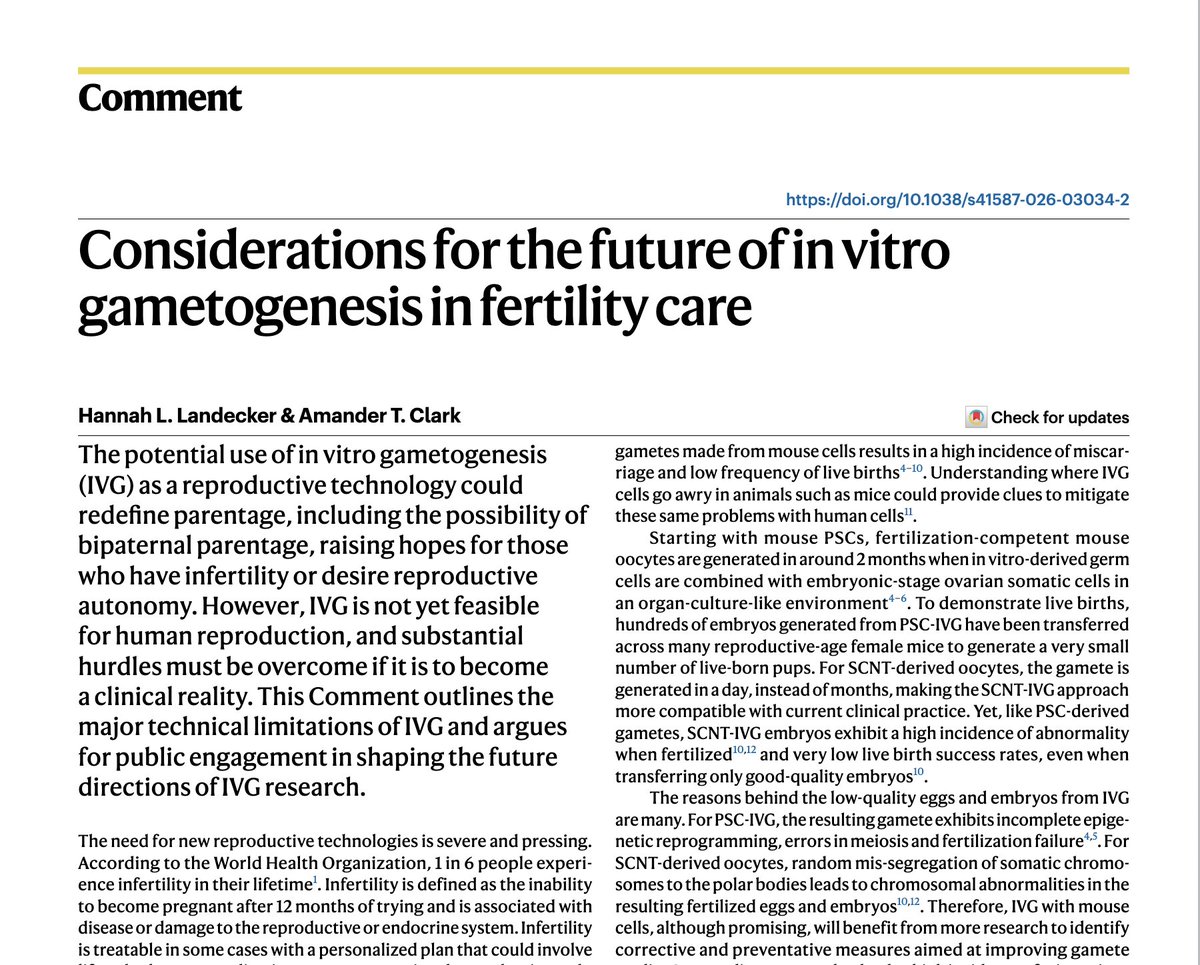
Excited to share our Review on human PGC development covering the latest in vivo observations & in vitro developments, particularly in the last 5 years. If you’re interested – have a read! journals.biologists.com/dev/article/15…
From: @astar_gis @karolinskainst @uniofwarwick @GurdonInstitute
English