Sabitlenmiş Tweet

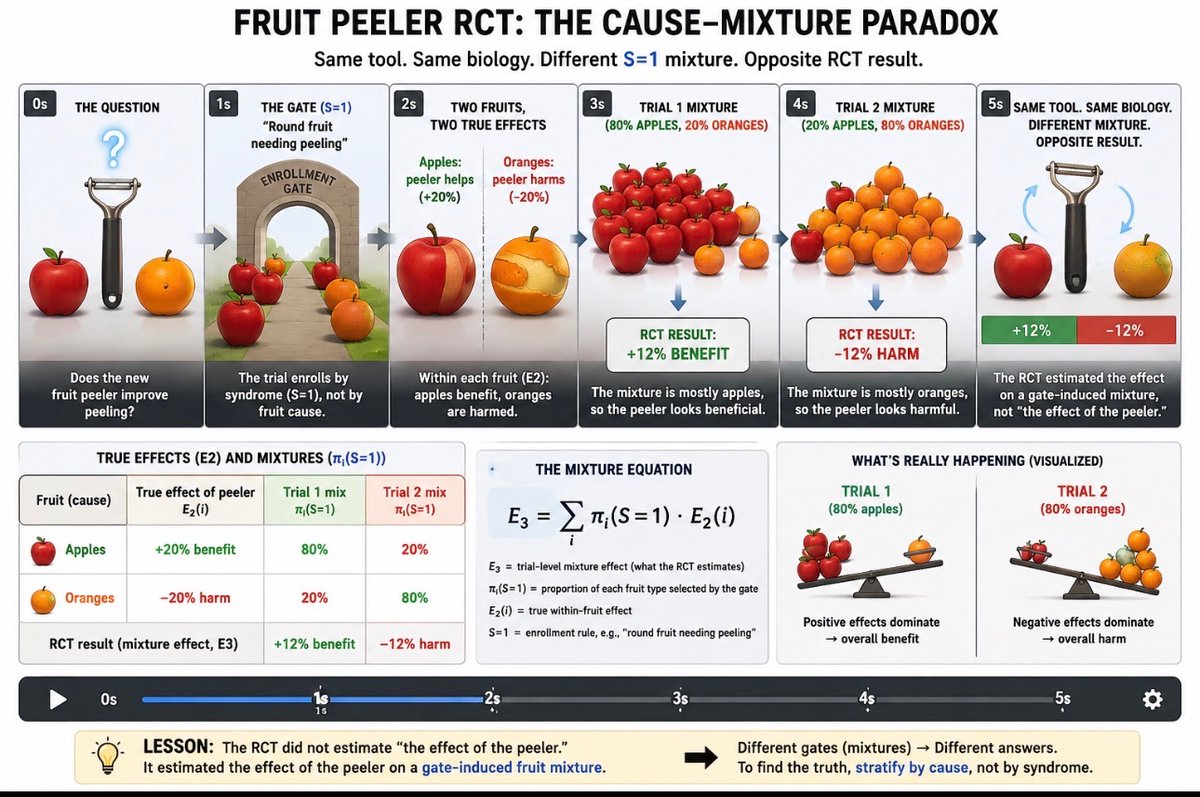
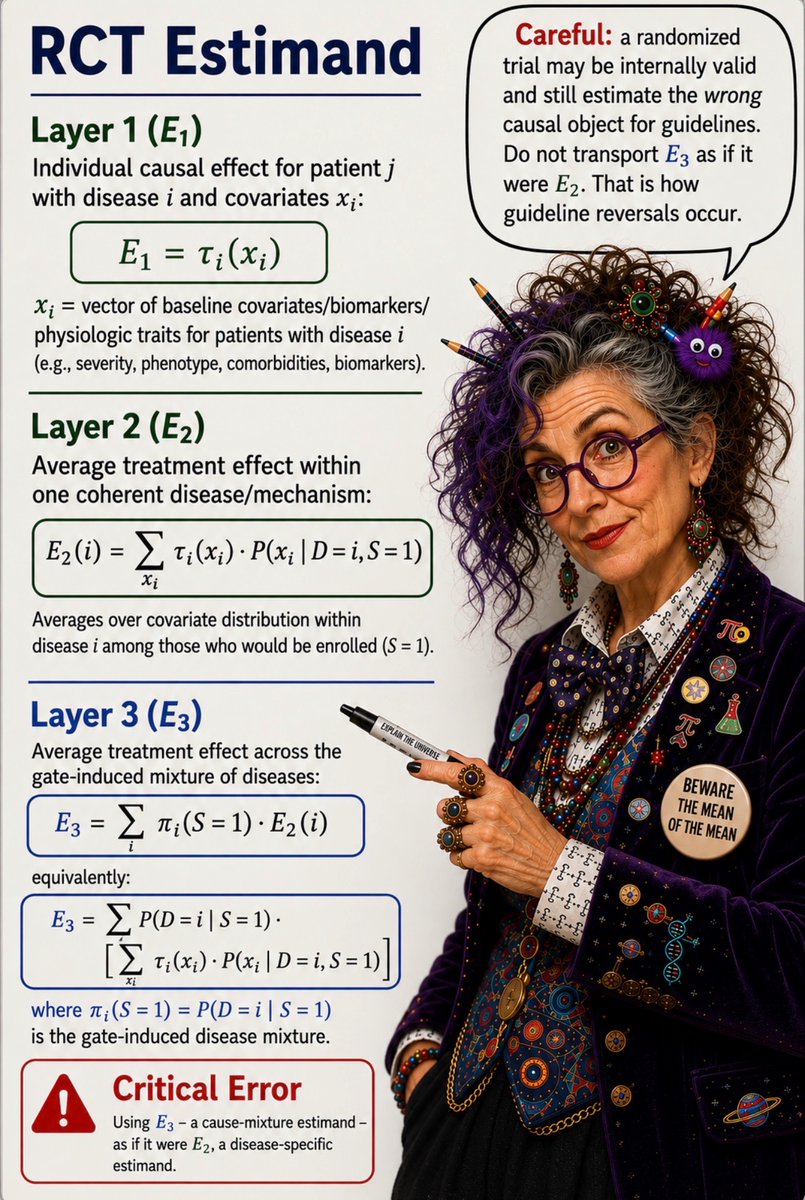
@fluidloading @bentatoo31 @Denis_Faust @Procto_Log The story of pathological consensus and shortcutting the RCT method of Hill/Fischer with the Petty/Bone science. The lumping paradigm.
The Physician’s War: The Story of the Hidden Battle between Physicians and a Science Based on Pathological Consensus a.co/d/8OtJlVk
English