Sabitlenmiş Tweet

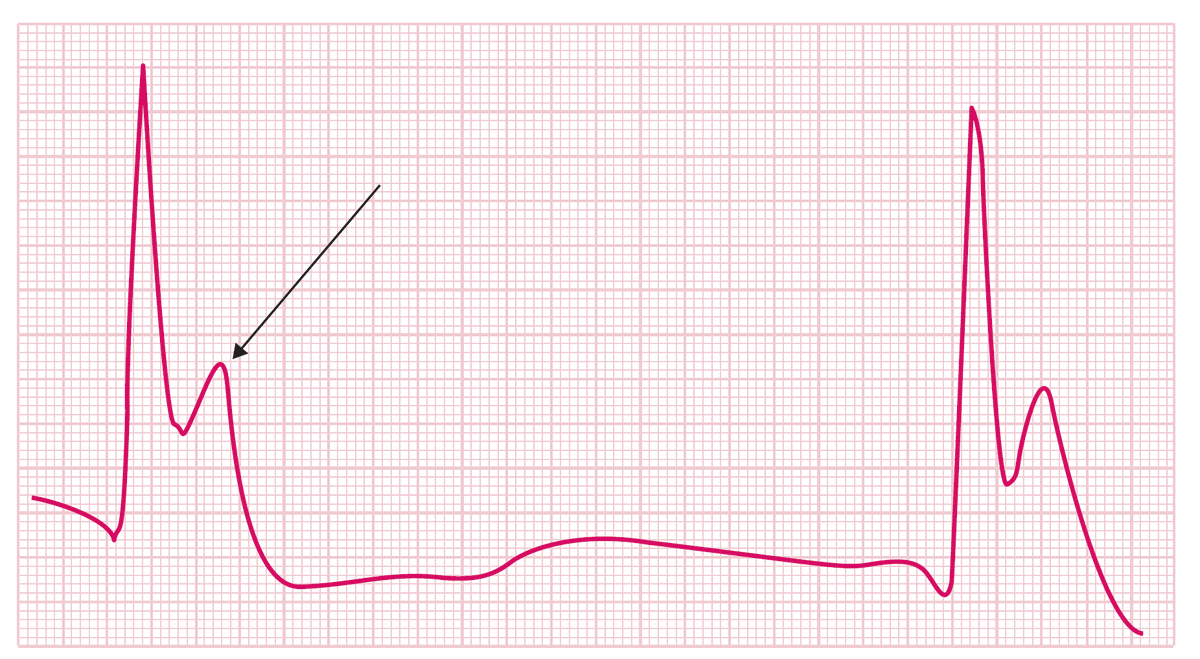
🛑 Stop guessing about Drug-Induced QT Prolongation.
Use QTMeds the 1st Privacy-First Prescription Analyzer.
📸 Offline AI to scan full prescriptions in seconds.
✅ Detects QT risks instantly.
🔒 100% LOCAL: No cloud upload.
🚀 Join the Beta (Free): [qtmeds.com]
English