RhondaHunter retweetledi

This should have a million retweets…literally. This is the moment to be loud, to be heard. We cannot let this govt trample any more of our rights. #saynotogerrymandering #stopthesteal
English
RhondaHunter
556 posts






I have learned that very senior govt officials have asked through back channels to try to muzzle my advocacy. 2/5


Apparently it’s okay now for an oil company (delinquent in payment to the landowner) to just help themselves to more land if they can’t reach a well site via their lease road. Land in foreground in photo used to get service rig, tank trucks etc. to the well site by trespass. 1n

The entire country should be paying attention to what's happening in Alberta. Nobody fights for landowners more than @mark_dorin. He talks to us about "deadbeat" oil companies, an ineffective Energy Regulator, and the toll gas leaks took on his own family.

Happy Pride night in Edmonton! 🌈🏒
Landowners Lock Out "Deadbeat" Oil Company x.com/i/broadcasts/1…

"We don't want to let a broke industry run the province. That's stupid." Landowners have no choice but to lock out "deadbeat" oil companies, says Polluter Pay Federation's @mark_dorin. How would you fix this mess? 👀 FULL: rtrj.info/031826Mark 🎧: rtrj.info/031826

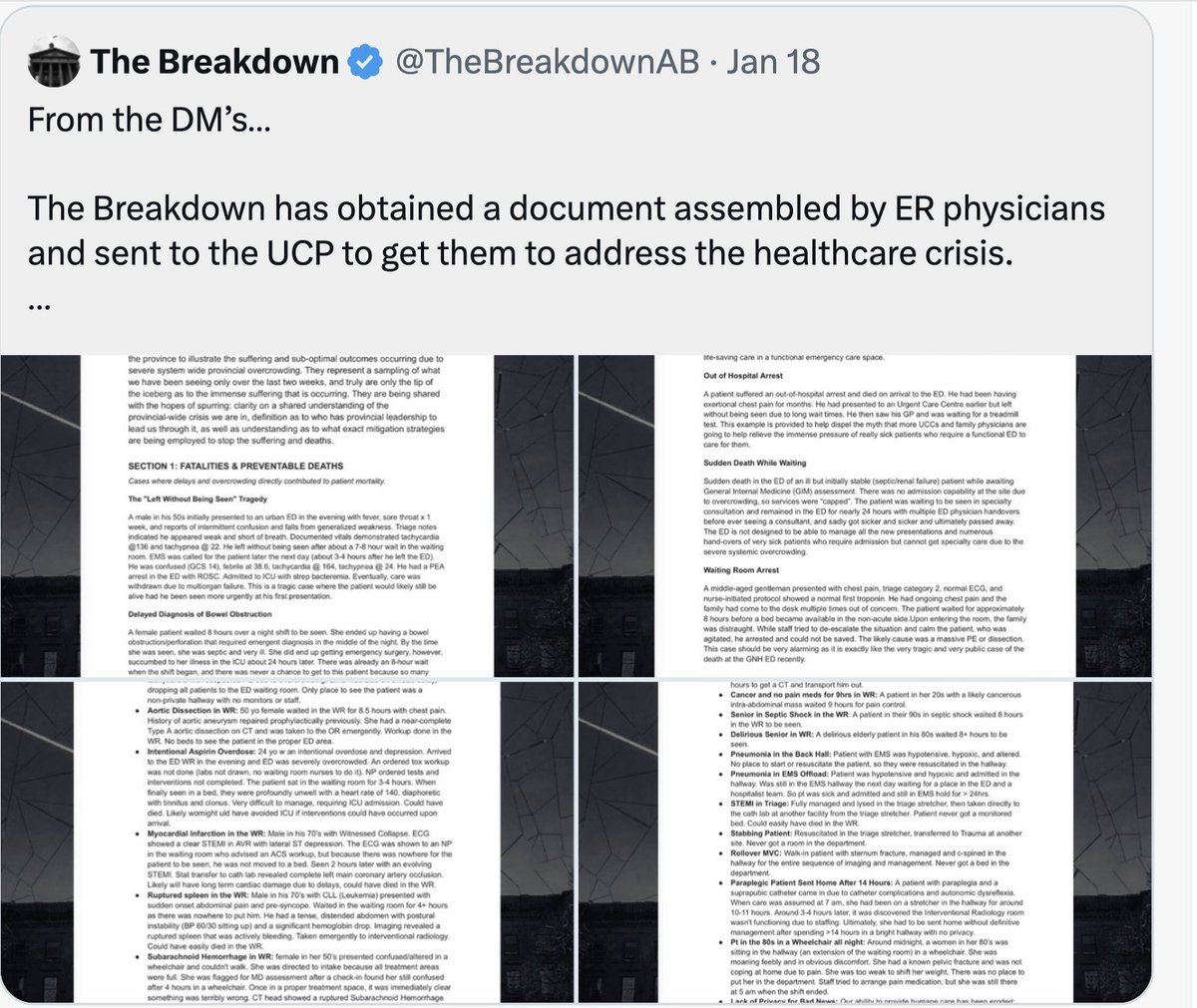


The Triage Doctor Role is a CRISIS and DISASTER protocol and when it is instituted, the whole health system is in crisis. The ER is "The Canary in the Coal Mine" and the Canary is Dead!. When the Premier says “it takes two parties to negotiate,” Albertans deserve full context. Over a two week period, out of approximately 500–600 emergency physicians who cover Alberta’s hospitals 24/7, and are there when you need us most, a small number recently documented 35–40 anonymized cases from across the province, including: • Patients who left without being seen and later died • Cardiac arrests occurring in hallways • Septic shock patients waiting 7–8 hours in waiting rooms • Aortic dissections and STEMIs managed in non-monitored spaces • Seniors in septic shock waiting 8 hours before assessment On February 1, Minister @MattJonesYYC announced immediate implementation of triage liaison physicians to protect patients in overcrowded emergency departments. It is now March 2, and the roles remain unfilled and Alberta's emergency departments are still in crisis. This is what delayed execution looks like. The TLP role is high-risk harm reduction: active surveillance of unstable patients in overcrowded waiting rooms. It is not a fix to the system FLOW crisis that remains unsolved my Minister @JasonNixonAB unable to move an adequate number of ALC's out of the hospital to get the system out of crisis. The TLP role requires: 1. A private, safe assessment space, not a hallway chair in front of 50–100 people. Albertans deserve privacy, dignity, and safety. 2. Dedicated nursing support (RN/LPN). Emergency medicine is team-based; physicians cannot safely do this alone. 3. Clear medico-legal structure. 4. Fair compensation in 2026 dollars for high-risk overtime work, not 2009 dollars. Seventeen years ago (2009-2014), emergency physicians performed this role at roughly 70% of their standard ER clinical rate. The proposal today mirrors that nominal rate despite dramatically increased system strain and risk. Emergency physicians are not refusing to help. Many are willing to step in and work overtime shifts at reduced rates, as we did before. There are many physicians who perform high-risk, after-hours work: ICU physicians, trauma surgeons, neurosurgeons, emergency physicians, etc. High-risk emergency care in the middle of the night is not compensated at 70% of weekday daytime rates from 17 years ago. If you call a plumber at 2 a.m., you don’t expect to pay weekday rates from 2009. In fact, they are offering the ER doctors close to the plumber's actual evening and weekend rate today. This is not about greed. It is about safety, structure, liability clarity, and sustainability. When patients arrest in hallways and septic patients wait 8 hours, negotiation delays are dangerous and they carry human consequences and legal risk for taxpayers. The broader issue is governance. Operational staffing, resourcing, and compensation models should be designed by hospital leadership and clinical experts, the people hired to run emergency departments safely, not directed through political offices. If a government announces a safety intervention and cannot operationalize it during documented patient harm, that is not a negotiation problem. That is a mismanagement problem and It is a leadership problem! Albertans dying in waiting rooms is tragic, but that is what happens when media personalities pretend to be experts in front line healthcare and interfere in day to day operations. Alberta has normalized unsafe access to emergency care. That is the crisis and Alberta families should be very concerned @ABDanielleSmith @nenshi @PfParks @JMeddings @ryanjespersen @TheBreakdownAB @cspotweet @Albertadoctors @UCPCaucus @Alberta_UCP @albertaNDP





