Sabitlenmiş Tweet
Ross Urry, PharmD
604 posts


Ross Urry, PharmD
@Ross_Urry
EM PharmD | Views are my own #TwitteRx #FOAMed
Utah, USA Katılım Eylül 2020
119 Takip Edilen112 Takipçiler
Ross Urry, PharmD retweetledi
modern IV contrast dye for CT scans isn’t neprotoxic.
definitive imaging saves lives.
this is so simple but people & journals & textbooks keep on messing it up.
Dr. Chacón-Lozsán F .'.@franciscojlk
🩻Contrast-induced AKI: one of the biggest myths still shaping clinical decisions For decades we were taught: 👉 “Contrast damages the kidneys” 👉 “Avoid CT with contrast in CKD” 👉 “Hydrate, protect, delay imaging if needed” But what if… most of this is wrong?🤔 ->The uncomfortable reality Modern evidence shows: 👉 Low-osmolar contrast rarely causes true nephrotoxicity 👉 Even in CKD, AKI, and ICU patients 👉 The risk is often overestimated—or nonexistent So where did the fear come from? 📍 1950s high-osmolar contrast (actually toxic) 📍 Poorly controlled observational studies 📍 “Creatinine rise = contrast injury” assumption 👉 Correlation became causation 👉 And the dogma stayed ⚠️What recent data tells us ✔ No difference in AKI rates with vs without contrast ✔ No benefit from bicarbonate, NAC, or aggressive hydration ✔ Even ICU and AKI patients show no worsening outcomes ->Translation to real life 👉 The patient was going to develop AKI anyway...Not because of contrast!! ->The real problem: “Renalism” 👉 Avoiding necessary imaging 👉 Delaying diagnosis 👉 Choosing inferior tests And that leads to: ❌ Missed PE ❌ Delayed sepsis source control ❌ Worse outcomes ->Clinical mindset shift Instead of asking: 👉 “Will contrast harm the kidneys?” We should ask: 👉 “Will NOT doing the scan harm the patient?” ->Who still deserves caution? ✔ eGFR <30 ✔ Severe hemodynamic instability ✔ Multiple nephrotoxins Even then: 👉 Optimize volume 👉 Minimize dose 👉 Don’t delay critical imaging 🤓Bottom line ✔ Contrast nephrotoxicity exists… but is rare ✔ The fear is bigger than the risk ✔ The harm of NOT imaging is often greater In critical care 👉 We don’t treat creatinine 👉 We treat patients And sometimes… 👉 The most dangerous thing is NOT the contrast 👉 It’s hesitation. 📃Reference Florens N, Demiselle J. Kidney360 7: 445–449, 2026. doi: doi.org/10.34067/KID.0…
English
Ross Urry, PharmD retweetledi


Ross Urry, PharmD retweetledi

Another 🔥 take:
There’s an overconfidence in clindamycin and its role in practice.
For most indications:
A) better options often exist (linezolid)
OR
B) better questions should be asked (are you REALLY allergic to the primary treatment options?)
AND
C) resistance a problem
English
Ross Urry, PharmD retweetledi

2025 ACC/AHA/ACEP/NAEMSP/SCAI Guideline for the Management of Patients With Acute Coronary Syndromes #AHAJournals
ahajournals.org/doi/10.1161/CI…
English
Ross Urry, PharmD retweetledi

The pros and cons of methylene blue in septic shock. Although I do not feel that this is ready for prime time, I’m happy it is being discussed. There’s an entire chapter to this topic in “The Vasopressor & Inotrope Handbook”. 🎩 tip to the authors.
eddyjoemd.com/foamed/

English
Ross Urry, PharmD retweetledi

📣📣 PGY2 CC Candidates 📣 📣
Looking for flexible and diverse learning experiences to strengthen your CC/ED experience and knowledge?
Come PPS with @UMMCPharmacy :
careers.ashp.org/jobs/20706407/…
#PharmICU #TwitterX #pharmacy

English
@apothecary_aly Yes and I know other hospitals have interpreted it that way as well
English

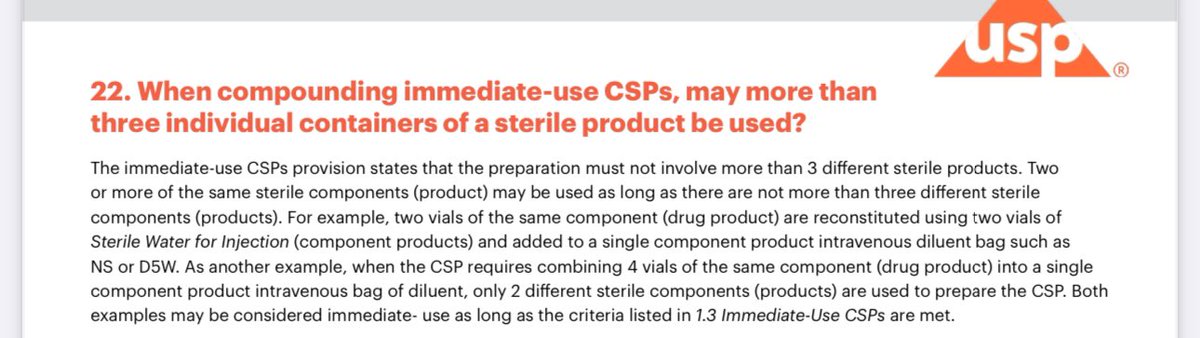
@Ross_Urry I think this may be what you’re referring to. I agree it sounds like as long as it’s the same product into 1 syringe then it’s considered okay is my interpretation
English
For those that IV push Keppra > 1.5g, how do you remain compliant with USP 797 given the number of vials exceeds 3? Trying to make the most of an IV fluid shortage lol #PharmICU #TwitterRx #NeuroICU
English
@Ross_Urry I’ll take a look there! I rec’d the change today and was told we couldn’t because “it’s more than 3 vials.”
English
Ross Urry, PharmD retweetledi

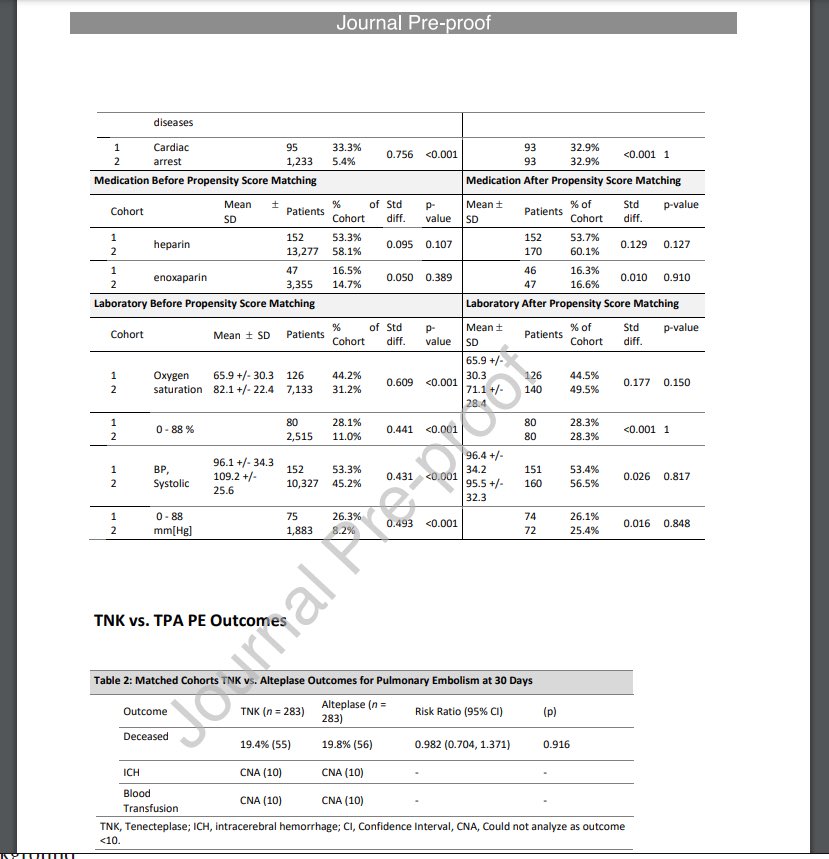
New article in-press showing no diff in outcomes between TNK and tPA for PE patients. Almost 300 pts in each group after matching which is pretty good imo. We’re doing TNK for AIS here but still doing tPA for PEs. Maybe this can change that?
jem-journal.com/article/S0736-…
English
Ross Urry, PharmD retweetledi
3 daily rants in one week? A new record!
It's a fair question. And the answer is, no. Even in immune suppressed patients there is no evidence that cidal vs. static means anything. Why?
Cosmina Gingaras MD, MPH@CosEpiID
@BradSpellberg @DrToddLee @ABsteward Can I ask whether the old-fashioned concept of static and cidal has any bearing in choosing antibiotic regimens in severely immunosuppressed patients?
English
@propofolpapi661 @AJWPharm @NG_Panos @PCC_PharmD @GilbertPharmD @PharmD_intheED @PharmacyToDose Definitely frustrating at times. I’ve been told that if there is blood noted on imaging then to not start any anticoagulation while inpatient, regardless of if the bleed is stable or not. Sometimes is even difficult get DVT ppx initiated in high risk trauma patients
English
@AJWPharm @NG_Panos @PCC_PharmD @GilbertPharmD @PharmD_intheED @PharmacyToDose It’s just not done routinely at my shop. We don’t have the brightest minds in ICU and neuro. We’re a non academic community site with a lot of private community docs. Hard to get anything evidence based done
English
A very interesting slide from a wonderful AZ MSL showing similar rates of thrombotic events between AA and usual care among pts who got at least 1 dose of VTE ppx
Buuuuuuuuuuuut, if you don’t give VTE ppx, check out the footnote for rates of TEs …

English

okay it’s time to discuss ANNEXA
English

@DrSandman11 They sooooo missed the opportunity to call it “Roc-off”
English
@DrugInfoGeek Could you also hide the drugs from appearing on search unless they use at least 4 letters? Valc-/valg- vs valt-/vala-? Issue I would probably see would be thinking valacyclovir is spelled valcyclovir
English

Anyone have some good suggestions to avoid the Valcyte vs Valtrex medication misadventure?
I'm only coming up with some cursory suggestions (below) but know that #TwitteRx may have some clever, next-level practices that hopefully they would be willing to share?🙏🥺
English
Ross Urry, PharmD retweetledi
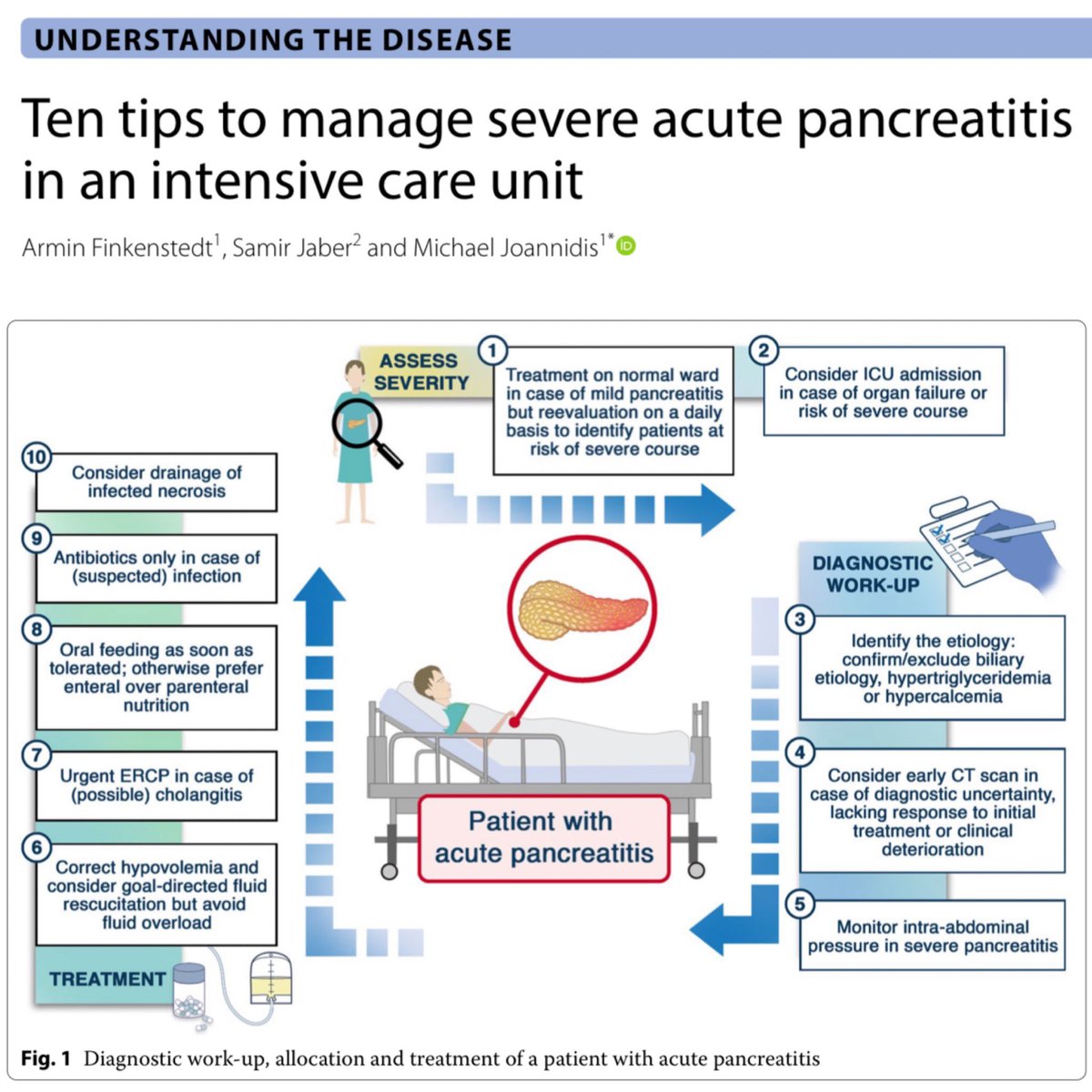
Manage severe acute pancreatitis like a pro! The days of just arbitrarily flooding patients with fluids and not feeding our patients are behind us. 🎩 tip to the authors.
eddyjoemd.com/foamed/
English
@AJWPharm @NLesh_PharmD How much LEV are you pushing at a time? 1500 mg? Or the entire 4500 mg?
English

@NLesh_PharmD No, but when they scan each vial it adds 500mg to the total dose administered so it's kind of an incentive to just scan all 8-9 vials unless they know to just type it in from the start. Hasn't been an issue as far as I'm aware haha
English
@AnotherPharmer Agree! Some of the smartest clinical pharmacists I have worked with either didn’t do a residency or just did a PGY-1
English

EM pharmacists—don’t pull the ladder up after you.
If you today won’t consider the CV of you when starting out…why?
PGY2 and BCEMP aren’t everything—you have to have ED experience to even sit for the BCEMP.
Consider a holistic approach when evaluating EM job candidates. 1/3
English