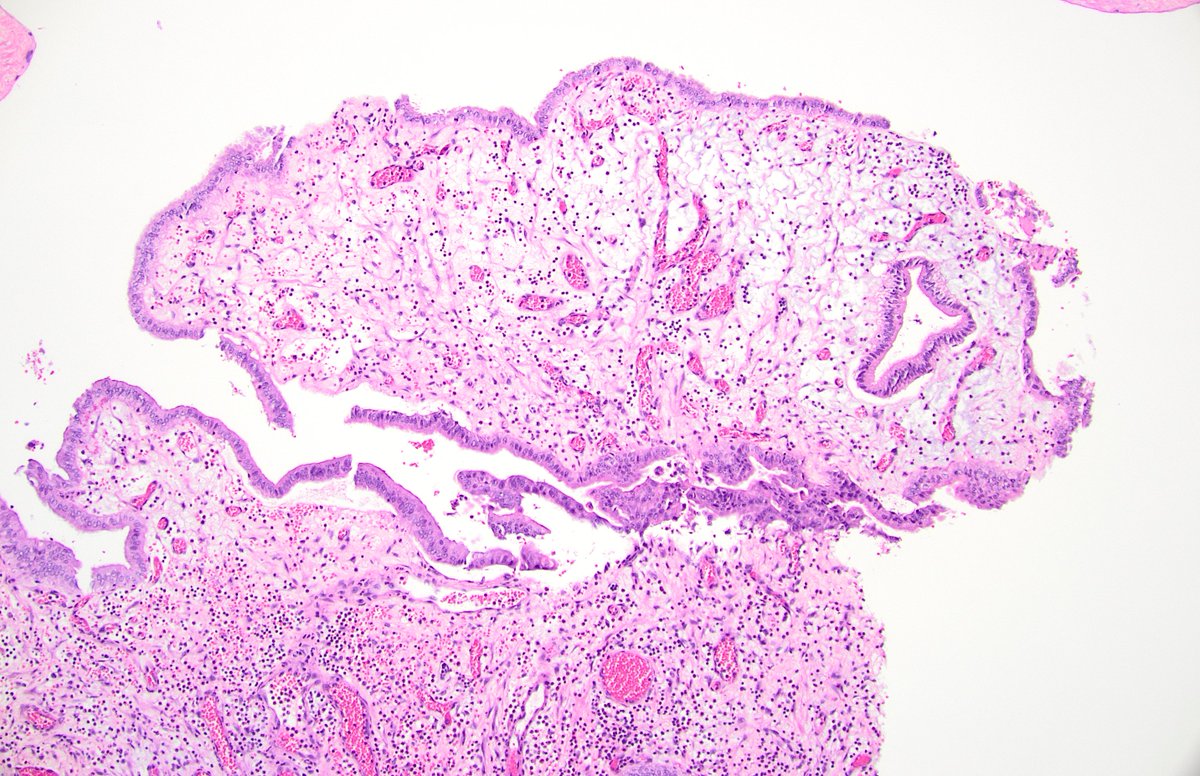
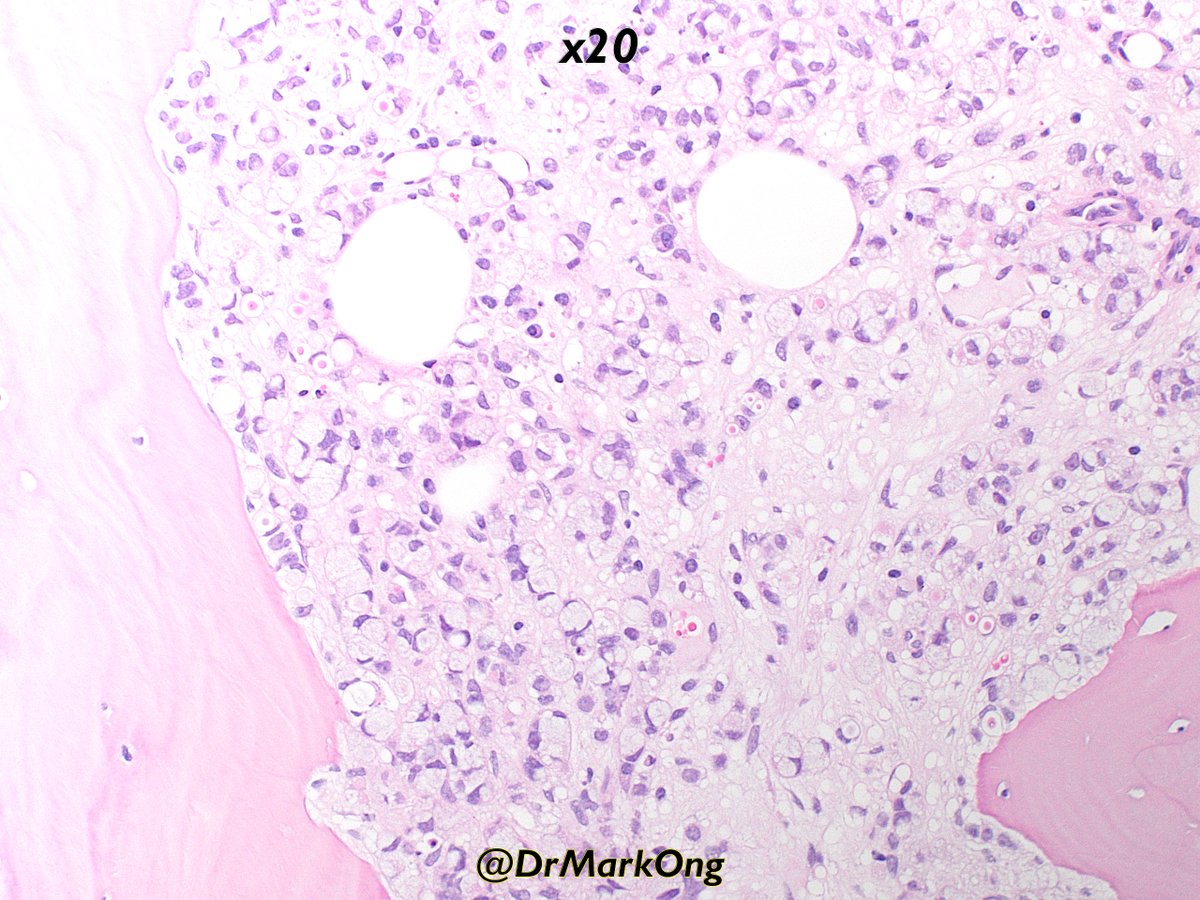
@forthejon @et565 On morphology I would have gone for HG dysplastic naevus. PRAME and molecular seem to point in the same direction here and what you have said is v reasonable. Management is the same - wider excision.
English
Jamie Sington
1.9K posts
@SingJamieD
UK Consultant Histopathologist






#WhatsNewInDermpath Utilizing PRAME expression and a meta-analytic framework for iSALT to explore atypical late-onset nevi of the elderly and their relationship with lentiginous and nested nevoid melanomas journals.lww.com/amjdermatopath…