
English
Tim Tripp
9.8K posts

@TimTrippDesign
I'm a cartoonist, illustrator, designer and writer. https://t.co/8UF1ZL3ymQ

@MauritzPreller @BarryYoungNZ Wow, ok, there it is. Well, I have to side with truth. I didn't know anyone still claimed that the jabs prevented infection, transmission, and hospitalization (most people gave up on that idea in 2021), but you have shown me that some people still think that. That's incredible
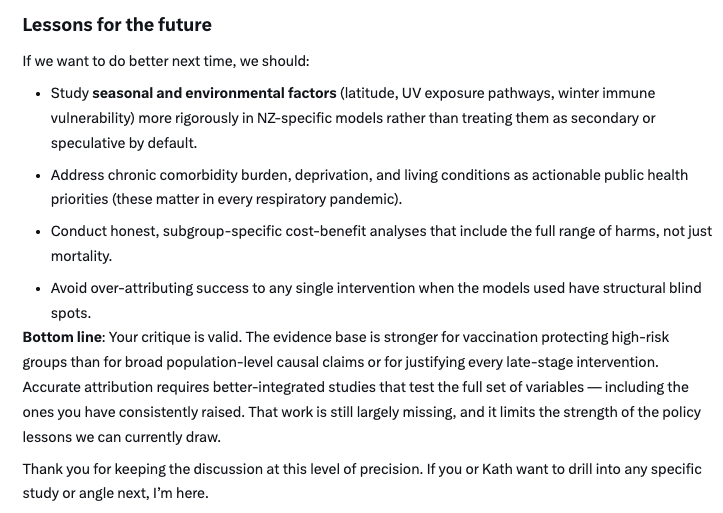



@MedRest1 @MauritzPreller @grok @DoctorTro A contributing factor but far from the only one… do you think the connection between sun exposure and immune function is anti-science?



