Sama Hoole@SamaHoole
BREAKING: Scientists have discovered a food that meets every essential human nutrient requirement.
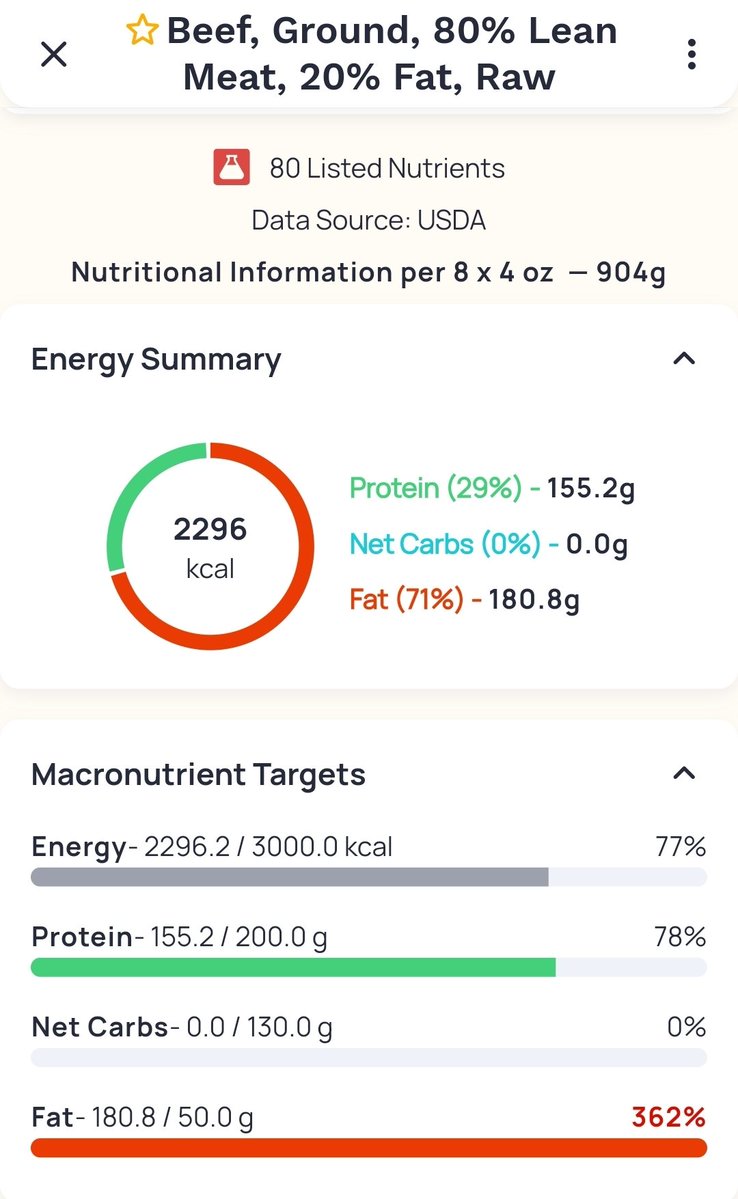
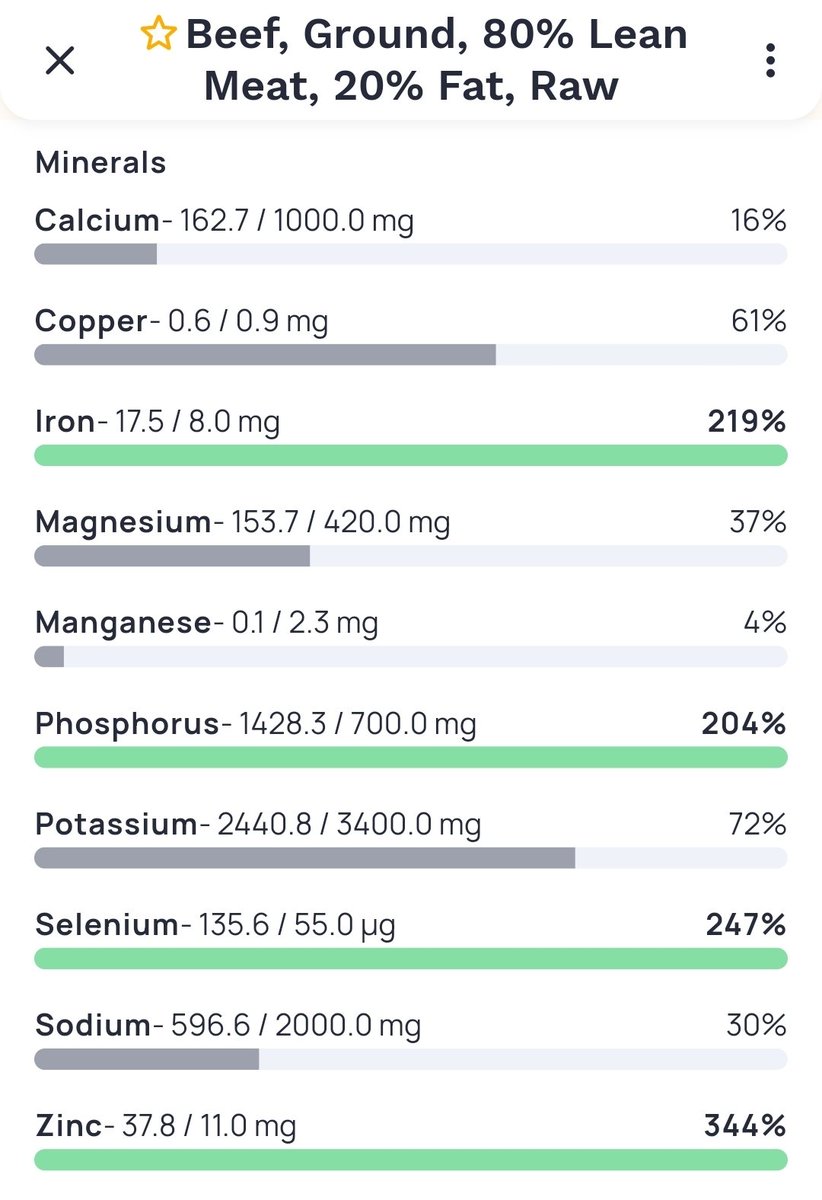
Complete protein with all essential amino acids. Active forms of vitamins A, D, E, and K2. Haem iron, zinc, B12, creatine, carnitine, CoQ10, choline, selenium.
No antinutrients. No lectins, oxalates, or phytates. No goitrogens disrupting thyroid function.
Requires no processing, no fortification, no chemical treatment. Apply heat. Eat.
No postprandial inflammation. No blood sugar spike. Exceptional digestive efficiency.
Available for 2.5 million years.
It is red meat.
The scientists did not actually discover this. It was just there.
We briefly forgot.