$NWBO Another day longer for patients, I asked Grok the greater MHRA concern - DCVAX-L efficacy or manufacturing:
Manufacturing consistency (part of the “quality” pillar in MHRA’s safety/quality/efficacy assessment).86
MHRA is currently reviewing Northwest Biotherapeutics’ Marketing Authorisation Application (MAA) for DCVAX-L (submitted December 2023, with a request for the rapid 150-day pathway for serious unmet needs like glioblastoma). As of late 2025, the agency has publicly confirmed it is actively assessing the application “rapidly for safety, quality, and efficacy” with no backlog issues, but it cannot comment on specifics during review.8662
No public MHRA statement singles out one area as the “greatest” concern (regulators keep application details confidential). However, the nature of DCVAX-L as a personalized autologous dendritic cell ATMP (Advanced Therapy Medicinal Product) makes manufacturing/quality the heavier lift compared with efficacy:
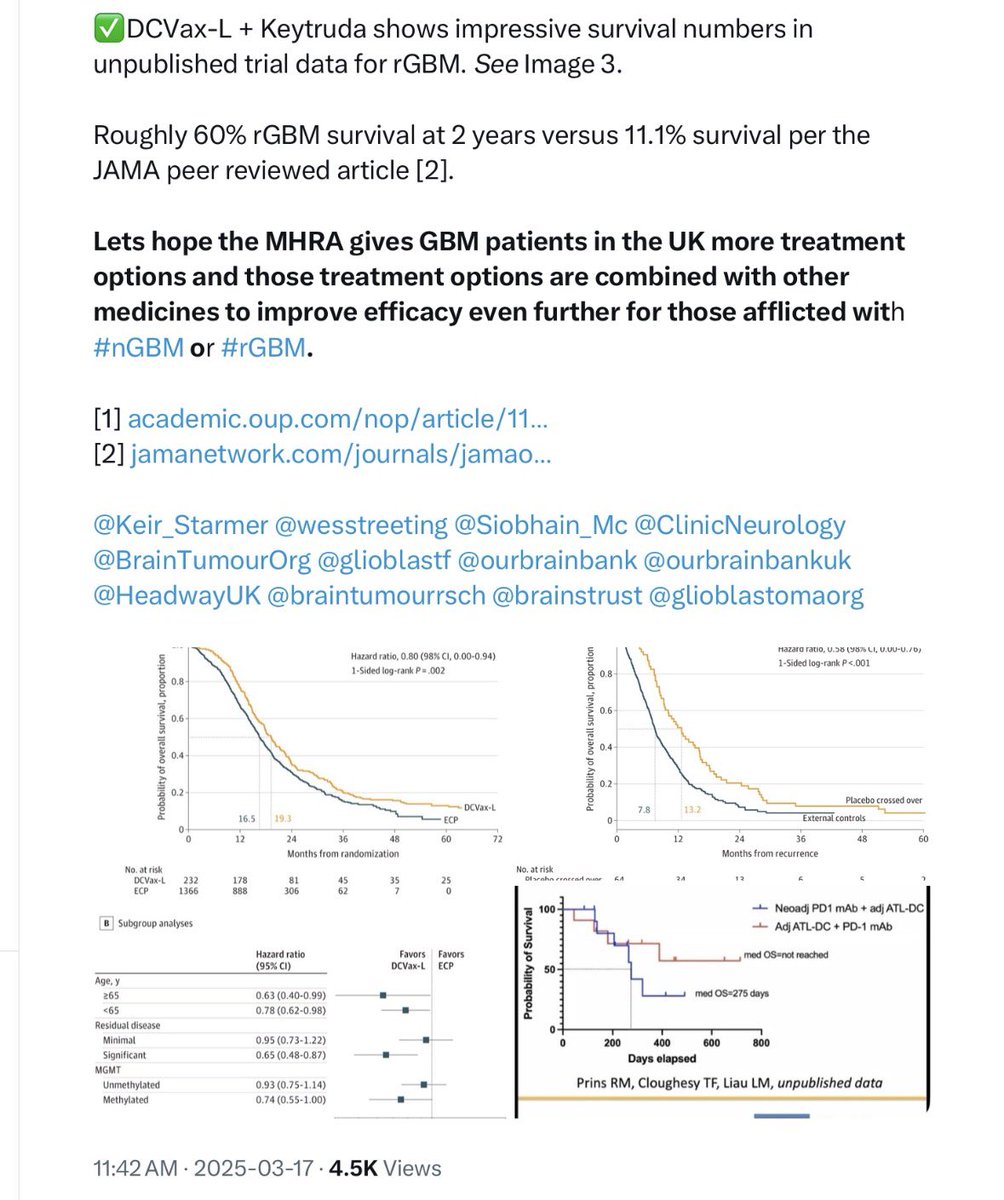
•Efficacy data is already strong and aligned with MHRA’s evolving frameworks. The Phase 3 trial (331 patients) showed statistically significant and clinically meaningful survival extensions vs. matched contemporaneous external controls (published in JAMA Oncology). MHRA has issued guidance supporting real-world data (RWD) and externally controlled arms (ECAs) for rare/unmet-need indications like GBM, and investor/regulatory analyses note this aligns with what NICE and MHRA have accepted previously.3010 There is no indication in public MHRA responses, parliamentary records, or company filings that the clinical data itself is the primary blocker.
•Manufacturing consistency/quality is the well-documented challenge for ATMPs like this. DCVAX-L uses a complex, patient-specific “living” process (leukapheresis + autologous tumor lysate-loaded dendritic cells, produced in ~8 days per batch with strict GMP, comparability, and release testing). For biologics/cell therapies, “the process is the product”—reproducibility, comparability, and control of individualized batches are core to the quality dossier. MHRA requires detailed GMP inspections of facilities, processes, quality systems, and validation as a prerequisite for MA.896
◦MHRA granted (and has renewed/expanded) GMP/Manufacturing and Import Authorisation (MIA) licenses for the key Sawston (Advent BioServices) UK facility specifically for DCVAX-L cell therapy production.187
◦Delays in ATMP reviews frequently stem from CMC (Chemistry, Manufacturing, and Controls) questions, comparability data, and manufacturing inspections—exactly as seen with other complex therapies (e.g., a BioMarin hemophilia A gene therapy faced a 180-day clock stop on manufacturing consistency; similar patterns appear in MHRA ATMP timelines).4885
◦Investor and analyst discussions consistently flag manufacturing comparability and decentralized/point-of-care scaling (e.g., via automated systems) as the key ongoing focus area for this personalized product.85
In short, the clinical efficacy evidence enabled the MAA submission and is being reviewed under modernized ECA/RWD pathways, while the personalized manufacturing process triggers the most intensive scrutiny, inspections, and potential clock stops typical of ATMPs. This is why manufacturing consistency is MHRA’s greatest (practical) concern for DCVAX-L approval. The review remains ongoing with no rejection or major efficacy red flags reported.
English