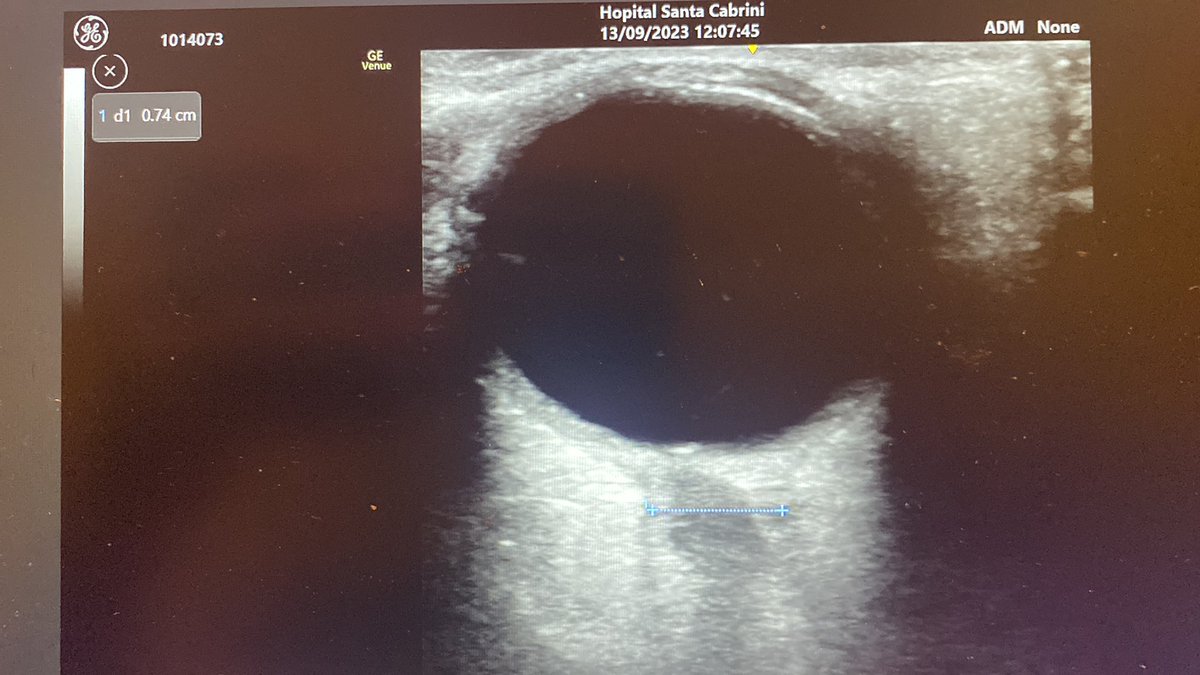
@ThinkingCC Great case. Take it opening pressures were quite high.
2 questions - 1. Any concerns re LP with ICP high? 2. ONSD wide but no Optic disc elevation?
English
Rob Devins
22 posts



#ILCOR #AdvancedLifeSupport Point-of-care Ultrasound is intuitively appealing to find reversible causes, but we don't actually know it helps 1/

#CanadaTruckers BLASTS #TruckersForFreedom2022 Says "It's RIDICULOUS - we need to be vaxxed" Want to bring it back & forth over the border Want a job? GET VACCINATED #TruckerConvoy2022 #FreedomConvoyCanada #TrudeauDictatorshipMustGo #TrudeauResign #TrudeauIsACoward #cdnpoli



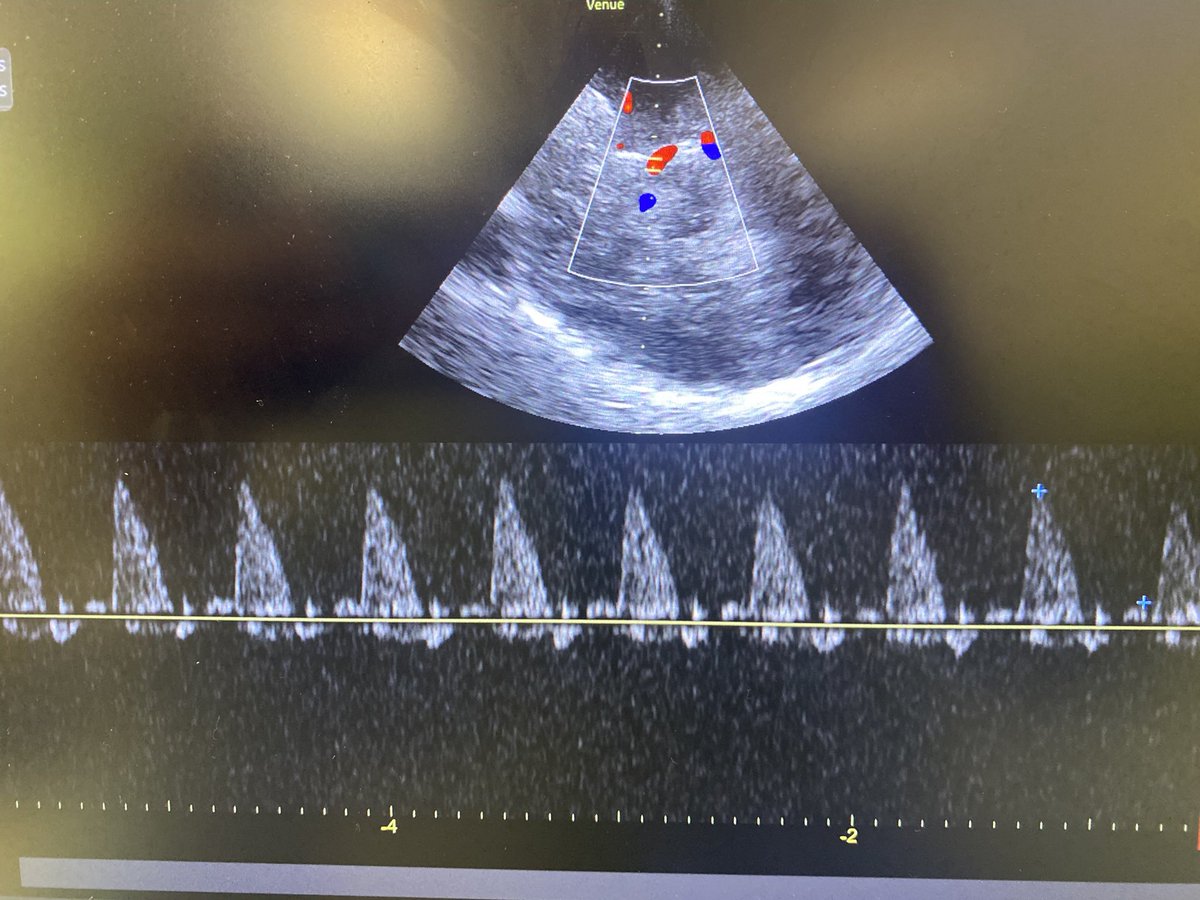
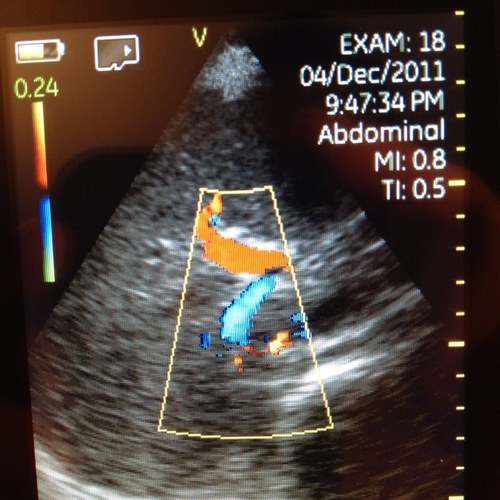
AKI in young pt with morbid obesity on mechanical ventilation and prone position (COVID-19). Cr 2.7 mg/dl. Persistent oliguria despite 2L crystalloid and Lasix gtt. BP 130/80. No vasopressor. CRT 1 sec. CPK 7000, K 6.7, UA: Blood +++, no RBC, SG 1.020, FENa 0.2% 1/
Introducing a new tool for research and education: PLUCK lets you extract a high quality still image from your ultrasound clip, annotate, and save it. Top journal download presets also included. Free to use. ultrasoundoftheweek.com/pluck/ #FOAMed #FOAMus
A rational approach to PE workup in pregnancy medscape.com/viewarticle/90… based on recent AnnIM article (Medscape registration free) #FOAMed @UMEmergencyMed