Sabitlenmiş Tweet

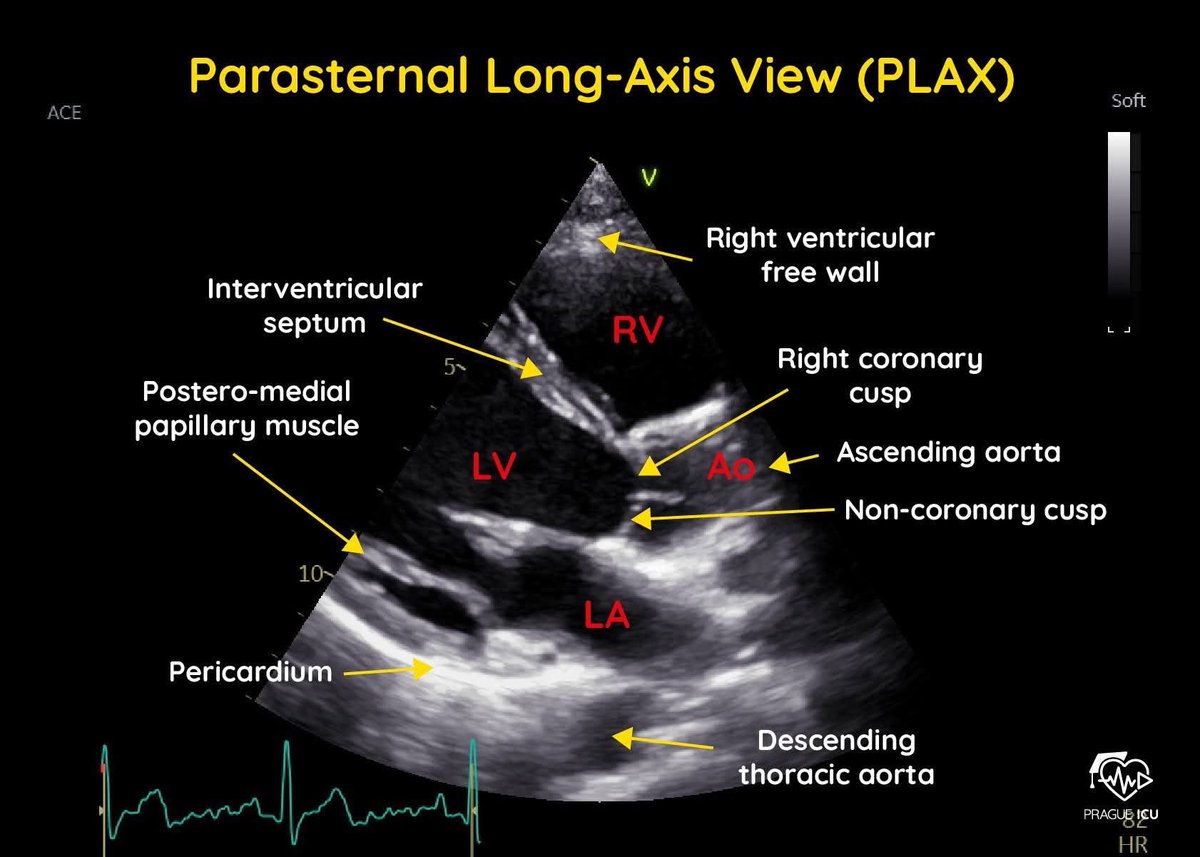
some says #POCUS answers (to the basic #FICE #CUSIC #FAMUS questions) are binary: yes/no.
but imo there must be 3:
- yes
- no
- i don’t know
3rd is not cool, but absolutely valid and most importantly: safe
Prof. Feynman@ProfFeynman
We need to teach how doubt is not to be feared but welcomed. It's OK to say, "I don't know."
English