
@s7saith @sunydownstate Looks like you had an amazing time at SCAI. Hoping to join you next year!
English
Harshith Chandrakumar
231 posts
@harshithpriyan
IC Bound | Chief Cardiology Fellow @ SUNY Downstate medical center ‘24 - ‘26 | Kelley Physician MBA | IM Chief Resident ‘23-‘24 | Food & Fitness enthusiast












Congratulations to Fletcher Bell and the publication team on their manuscript summarizing CalShock 2025. Thank you @LiannaSC, @CaliforniaACC, @RolaKhedrakiMD, and @adityadoc1 for your partnership and support without which this would not have been possible.link.springer.com/article/10.100…






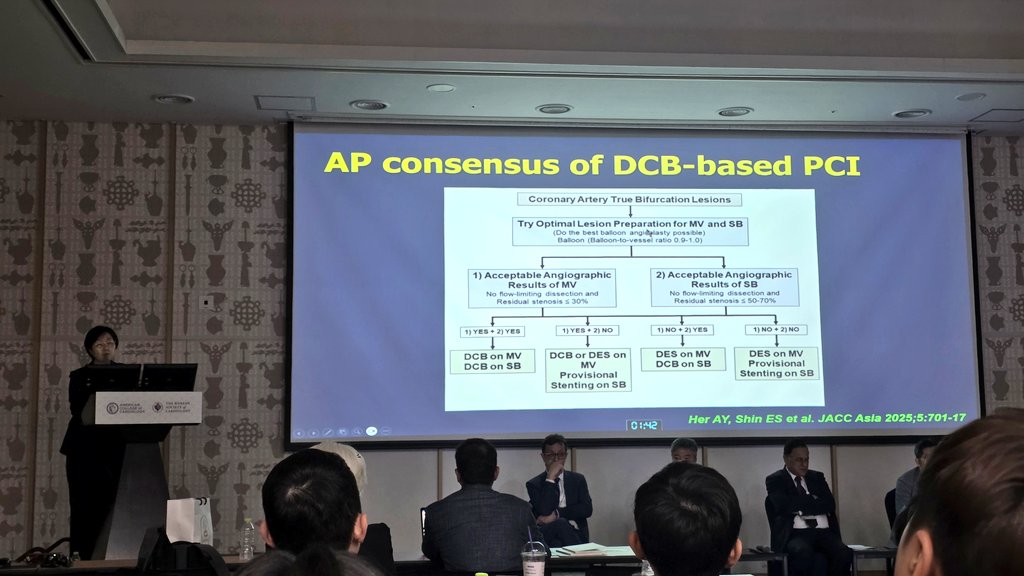



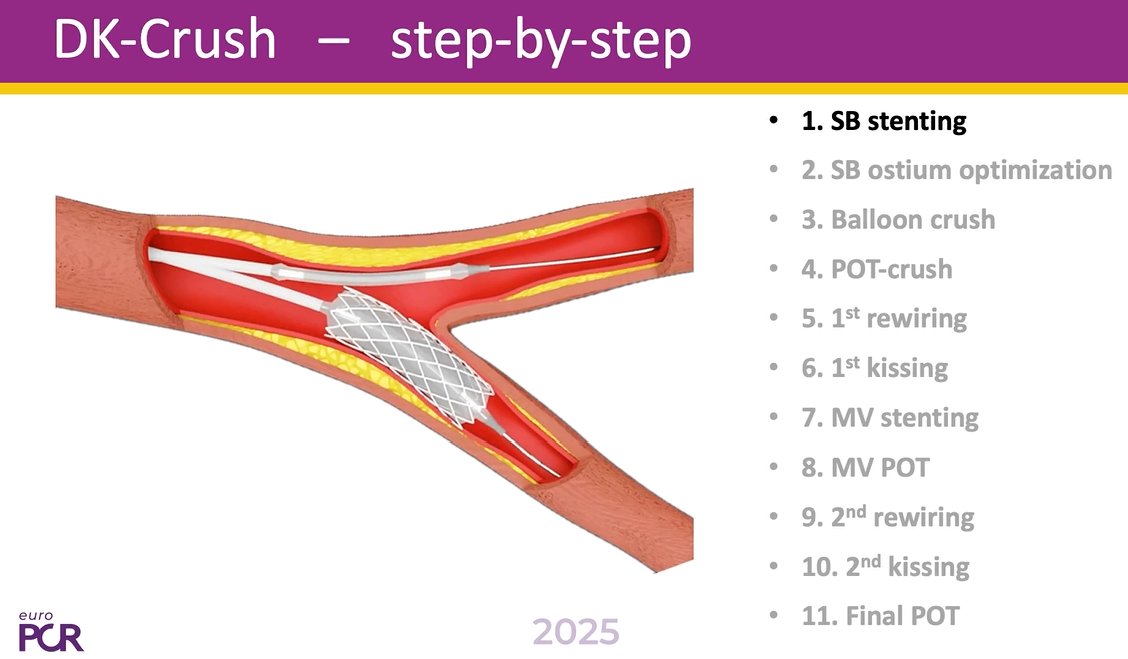




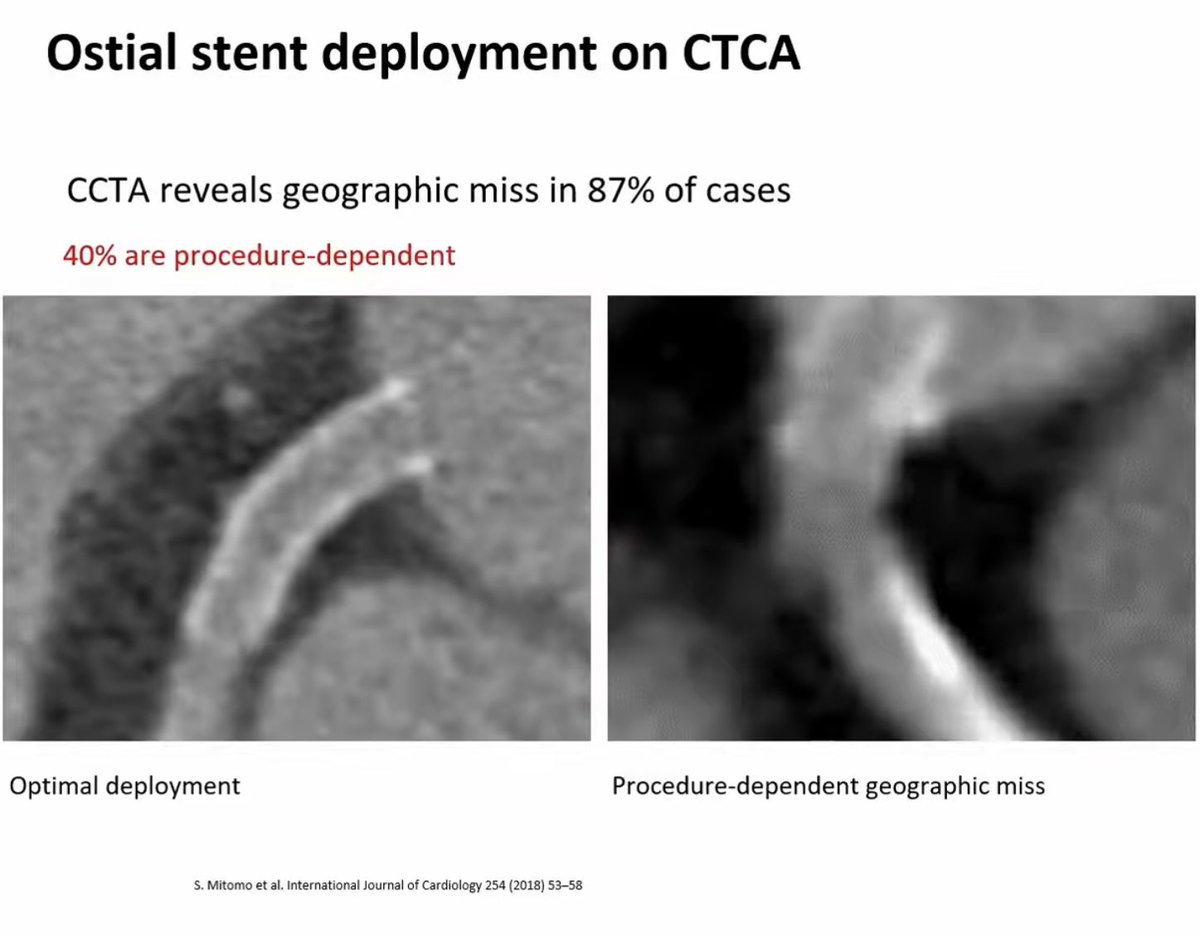



JACC Asia video on RTIG stenting for anyone who might find it helpful. Tips and tricks / steps / ivus interpretation jacc.org/digital-conten…

