HedgeSourced 🇺🇸🇨🇭 retweetledi
HedgeSourced 🇺🇸🇨🇭
5.1K posts


HedgeSourced 🇺🇸🇨🇭
@hedgesauce
I love long walks to the bank
Irvine, CA Katılım Nisan 2013
1.6K Takip Edilen457 Takipçiler

@nateberkopec All these takes are correct if we assume that development on coding models will stall at this point in time. However assuming the same, or even smaller, development slope makes the previous statement a reasonable assumption.
English

Crazy how backwards this is. The "yes guy" is now in infinite supply, just type `claude` and you've got a new one. The "no guy" is the one in demand: the one who points out all the problems with all the slop your slopcannons are trying to merge to prod.
snoopy jpg@snoopy_dot_jpg
this will end in tears btw
English
Starbucks CEO defends a cup of coffee costing $9
He says the customers needs to just not think about it as a $9 cup of coffee, you’re paying for the “experience” of getting a Starbucks coffee
“In some cases a $9 experience does feel like you're splurging, and then what that means is we have to make it worthwhile.”
He says Starbucks customers “want to have a special experience and regardless of what your income level is, in some cases, a $9 experience does feel like you're splurging — well, this is a really affordable premium experience”
How out of touch could a person possibly be…
English

Programming has always been one hell of a drug.
Coding agents removing its most annoying facets just cranks that up to 11.
English
@LorenAdler This is such an uninformed take it’s almost criminal
English

High hospital prices are the chief reason the U.S. spends so much more on health care than other countries.
If you want to improve health care affordability, hospital costs are a good place to start.
Bob Herman@bobjherman
Hospital CEOs are currently testifying in front on Congress. @ahahospitals just held its annual meeting, and @_daniel_payne caught this extremely candid quote from Chuck Schumer showing just how much lobbying power hospitals have. statnews.com/2026/04/27/for…
English
@RepJasonSmith @WaysandMeansGOP Straight from the Payer playbook
English

Our health care system is broken. These days, non-for-profit hospitals look more like hedge funds with hospital beds.
Today, @WaysandMeansGOP is holding a hearing with hospital CEOs as we continue our investigation into the health care empires that have raised prices and taken away access.
Politicians have refused to take on the health care empire and its lobbyists for too long. If we’re serious about lowering costs and expanding access to health care, nothing can be off-limits.
English
@fishstark @BenSasse In your world you are asking the government to intervene in his world he is asking for personal responsibility
English

All right @BenSasse, let's make a bet.
Let's divide the US in half. I'll let you pick which half.
In your half, you ban Candy Crush. In my half we institute 16 weeks of paid parental leave, universal childcare, & a restored child tax credit.
Let's see which has more babies.
60 Minutes@60Minutes
“We've stopped making babies. We've decided that being distracted by a dopamine hit around Candy Crush might be a good way to spend your time. Not if you're a full human," former Sen. Ben Sasse says in an extended interview. cbsn.ws/4cA1Jrp
English
@noahkaufmanmd Noah I admire what you are doing but the road ahead is filled with different challenges that the ER won’t prepare you for. I wish you the best (of luck).
English

I left the hospital. I left the ER. I created my own Clinic and my own thing in Denver.
I can’t tell you how wonderful it is to practice medicine now.
I’m in love with practicing medicine again. It’s changed everything for me.
Spread the word. Other docs should know.

English
@ecommerceshares @jennablan He was the Stece Ballmer of Apple
English

Got emotional thinking about Tim Cook stepping down. Truly an end of a remarkable era in human technology.
He took Apple from $108bn in 2011 to $416bn in revenue last year, and from 250m to 2.5bn installed devices. Incredible.
I hope he gets to dance.
English
@novaramedia This is what happens when you elect a child who has never worked a day in its life
English

New York City mayor Zohran Mamdani has announced the location of the city’s first publicly owned supermarket, marking a step towards delivering on his pledge to bring down the cost of food.
The city will spend $30m (£22.3m) on the store, which is due to open next year at a marketplace in East Harlem, Mamdani announced on Sunday during an address to mark his first 100 days in office.
He wants to open five of the stores - one for each of the city’s boroughs - before the end of his first term in 2029. They will operate without paying rent or taxes and pass those savings onto shoppers.
During his address, Mamdani rebutted neoliberal arguments about the effectiveness of publicly owned businesses.
"Some will insist that city-owned businesses do not work, that government cannot keep up with corporations," he said. "My answer to them is simple: I look forward to the competition. May the most affordable grocery store win."
Mamdani has been quick to deliver on several of his major campaign pledges – many of them aimed at bringing down the cost of living – since taking office on 1 January. He announced the introduction of a free childcare scheme, intervened on behalf of tenants living in poor conditions and secured millions of dollars of restitution for workers.
Former presidential candidate Bernie Sanders made a surprise appearance at Mamdani’s address.
"I know that the mayor has been criticised and some say this is a radical idea," he told the crowd. "I'll tell you what is a radical idea: Giving tax breaks to billionaires. Throwing people off health care. That's radical. What's radical is starting a terrible war. That's radical. But providing affordable food to working families? That's not radical, it's exactly the right thing to do."

English
HedgeSourced 🇺🇸🇨🇭 retweetledi

California is trying to pass a bill that would criminalize investigative journalism with misdemeanors, $10,000 fines, imprisonment, and content takedown.
The proposed bill is titled AB 2624 and was made after I exposed mass fraud by immigrant groups in America.
Under AB 2624, government-funded entities like the Somali “Learing” Daycare centers would be protected from being exposed if they operated inside California.
The enemy truly is within. When our politicians would rather protect fraudsters and illegal migrants, it’s time for us to stand up or face mass oppression from the traitors who “rule” over us.

English
It’s funny. Now that I’m opening my own clinic, I’ve never wanted to practice medicine more! No more hospital administrator looking over my shoulder. No more dealing with insurance. I get to make all of the decisions, and I’m barely going to have to touch a keyboard or a mouse.
I just get to take care of patients which is my fundamental calling.
It’s unreal, and I can’t tell you how excited I am to finally practice medicine on my own terms!

English
@NeilFlochMD Current recession will decrease that number further
English

I am often mocked by my Wall Street friends when I tell the story of the “collapse of American medicine”. It is a direct result of two laws: 1. HITECH act of 2009 that implemented excessive cost and regulations on private practices and 2. ACA “Obamacare” law implemented in 2010. The cumulative effect of these laws was:
1. The collapse of the longstanding doctor-patient relationship as “you could NOT keep your doctor.”
2. The progressive financial failure of private practice physician who eventually joined hospital systems and private equity to reduce their debt.
3. Increasing cost of medicine as more physicians were working under the benefit of additional payments that include a “facility fee” which is awarded the hospital systems and not private practitioners.
4. The increase in administrative costs as increase regulations are a characteristic of large hospitals systems and uncontrolled and government-backed insurance mandates.
The above must be reversed in order to re-establish private practice in America.
Dutch Rojas@DutchRojas
15% of physicians remain in unaffiliated private practice. In 2010 that number was 75%. The physicians still standing are the ones who held out the longest. They don’t need employment. They need an economic structure that makes independence durable. That is a very large and very underserved market.
English
@noahkaufmanmd @KaufCare Will this get reimbursed? CPT codes?
English
DOCS: we have a great new rapid test that just got approved that we will be using @kaufcare and I suggest you read the following and look into utilizing this for your patients 👇
Russ Shaw MLS - Lab Scientist@RussellShaw_MLS
This is directly in my lane and I think FebriDx is one of the most important CLIA-waived diagnostics to hit the market in years. For everyone else reading this, here’s what it does. FebriDx is a rapid fingerstick test that measures two biomarkers simultaneously. CRP (C-reactive protein, which rises with bacterial infection) and MxA (myxovirus resistance protein A, which rises specifically with viral infection). One drop of blood. Ten minutes. The combination of those two markers tells the clinician whether the patient’s immune response looks bacterial, viral, or neither. The NPV is the number that matters most in practice. A 97% negative predictive value for bacterial infection means that when FebriDx says it’s not bacterial, it’s right 97% of the time. That’s the number that gives a physician the confidence to say “we’re going to watch this for a few days” instead of writing the antibiotic prescription just in case. The “just in case” prescription is how we got to where we are with antibiotic resistance. The CLIA waiver that just came through last week is the game changer. Before the waiver, FebriDx could only be run in moderate or high-complexity labs. That means a hospital lab. With the waiver, it can now be run in any CLIA-waived setting. Urgent care clinics. Physician offices. Retail health clinics. Long-term care facilities. The test goes from 18,000 eligible sites to 270,000. That’s a 15x expansion in access overnight. For your clinic specifically, this slots in perfectly with the shared decision-making framework we were just discussing. The physician presents the patient with the probability assessment. FebriDx narrows that probability in ten minutes with objective data. The 33% chance antibiotics help becomes either 80% or drops to under 5% depending on what the test shows. The prescription decision gets made with data instead of a guess. Antibiotic stewardship improves. The patient understands why they’re getting or not getting the prescription. Everyone wins. Get it for the clinic. This is point-of-care diagnostics doing exactly what it should do. Putting actionable lab data in the hands of the clinician at the moment the decision is being made instead of three days later when the culture results come back and the Z-pack has already been started. Don’t wait for the diagnosis. Read the label.
English

NASA pilot Victor Glover CLAPS back after being asked what it means to be the first black man to visit the moon: “It’s the story of humanity, not black history, not women’s history, but that it becomes human history.”
“I also HOPE we are pushing the other direction that one day we don’t have to talk about these first. That one day, this is just—and listen to this—that this is the human history.”
English
@SicNTiredYall @MaryBowdenMD @NBCNews You can’t hire physicians (regulation driven shortage) and have too many uninsured (also regulation) in rural towns. Remove regulations and hospitals will come.
English

@MaryBowdenMD @NBCNews Isn't it funny how the non-profit hospital systems avoid small rural towns? Maybe it has something to do with making money after all
English

More than 400 hospitals across the U.S. are at high risk of closing or cutting services because of the Medicaid cuts in President Trump’s “big, beautiful bill,” according to an analysis from the progressive watchdog group Public Citizen. nbcnews.com/health/health-…
English
@MaryBowdenMD @NBCNews Donations subsiding inadequate payer fees
English

@mcuban Problem is the Payers not the Providers. You’re falling into the propaganda trap blaming hospitals when the fault is with Payers and regulation.
English
HedgeSourced 🇺🇸🇨🇭 retweetledi

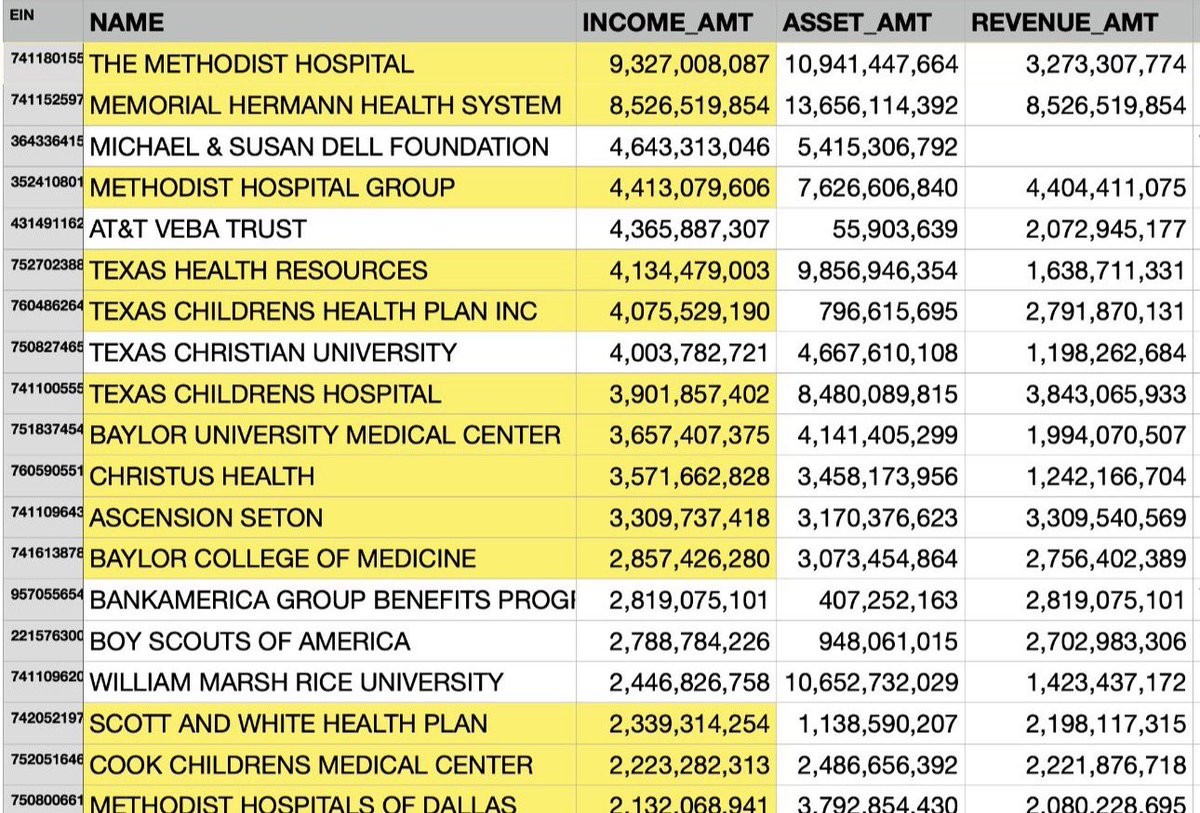
Why aren’t any of these at risk hospitals publishing their full accounting so everyone can see where they spend their money ?
All but one group of hospitals that I have looked at potentially investing in, spend so much on consultants and fees that it’s no wonder they are at risk
Plus, I have NEVER seen an industry that is worse than hospitals when it comes to buying medications and items like implants, screws, other devices. They overpay for everything.
And then when you show them how to save money, their “supply chain” employees resist any change.
They are so set in their ways, it’s a shock more don’t go out of business.
Prove me wrong.
NBC News@NBCNews
More than 400 hospitals across the U.S. are at high risk of closing or cutting services because of the Medicaid cuts in President Trump’s “big, beautiful bill,” according to an analysis from the progressive watchdog group Public Citizen. nbcnews.com/health/health-…
English
@paolino Thanks for the feedback. I found that using some particular skills drastically improved performance. Thanks for all your work on RubyLlm. It’s amazing
English
@hedgesauce I don't use any skills!
Just Voxtype for dictation, and the tmux setup by DHH on Omarchy.
Funny enough was just wrestling with Claude again not fixing a bug for an hour. Codex one shotted it.
English
I've been watching this since the first Codex dropped. There's no comparison. Codex is miles ahead of Claude Code.
But the narrative won't stop. Which tells me people didn't actually try Codex before confidently declaring a winner.
Even Opus 4.6 on max effort hallucinates constantly, confidently. Not on maxed out contexts, on fresh conversations.
Today: hallucinated results it should have searched. Blindly changed one without verifying. Searched but got the wrong answer. Then doubled down on a mistake it already made. Just a mess. 20 minutes for a simple row of feature comparisons.
Codex: searched everything, found nuance, suggested ways to represent it in the table. One shot.
English