José M Peñaloza retweetledi

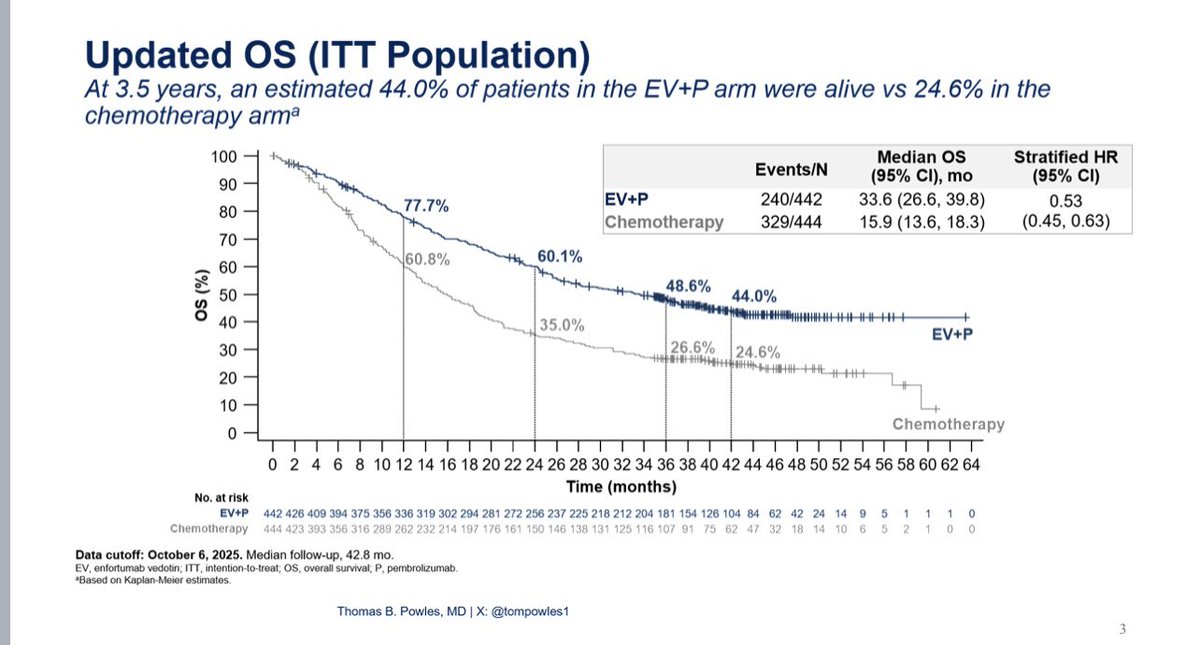
The 3.5yr OS from EV302 continues to show transformative benefit (HR 0.53 (0.45-0.63)) #ASCO26 for EV/pembro. The landmark OS for the CR population (30%) is ~90%. Median time to CR is 4.5 months (responses mature over time). Response rates of platinum chemo after EVP is 21% (OS 11 months). This should be considered a 2nd line standard. Median duration of EV was 7 months - longer in responders. Optimal duration of EV trials are needed. @OncoAlert



English