@CardioBeat_ You stole this image from @willyhfrick. Posting someone else’s image is OK if you get permission and give attribution, but to put it forth as your own is deceitful.
🧵 “The IV fluids didn’t save her. They erased her sodium.”
Today, let me introduce you to Anita.
Anita came to the ER with vomiting and mild dehydration.
Vitals stable. Mentally alert.
Labs: Na⁺ 134 mEq/L — almost normal.
She was started on “routine IV fluids.”
By morning, Anita was confused.
By afternoon, she had a seizure.
📉 Na⁺ 118 mEq/L
What went wrong? 👇
V-E technique is associated with better tidal volumes and reduced failure rates compared to C-E technique.
Wet Clinic at Vicente Sotto Memorial Medical Center
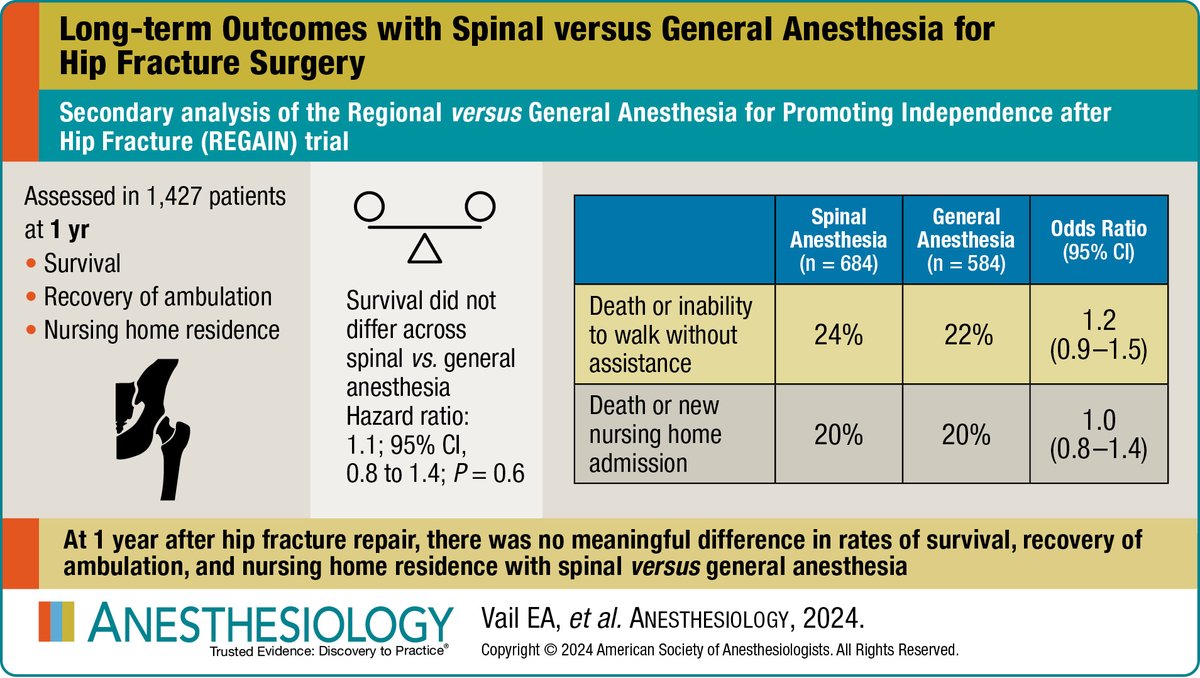
@_Anesthesiology Maybe i am missing something, but how does choice of anaesthesia affects long term outcome as compared to patients frailty, mrs, surgical technique, rehab plan etc...?
@DrRazi4@The_Iron_grey@ecgandrhythmRoe@EcgsOnly@smithECGBlog@EcgOxford How do i know there is reperfusion at posterior leads?
There seems to be combination of 1st degree hb and mobitz type 2. So would it qualify as high degree av block?
If there are q waves at inferior leads, when can we say it to be lafb? Or we just dont?
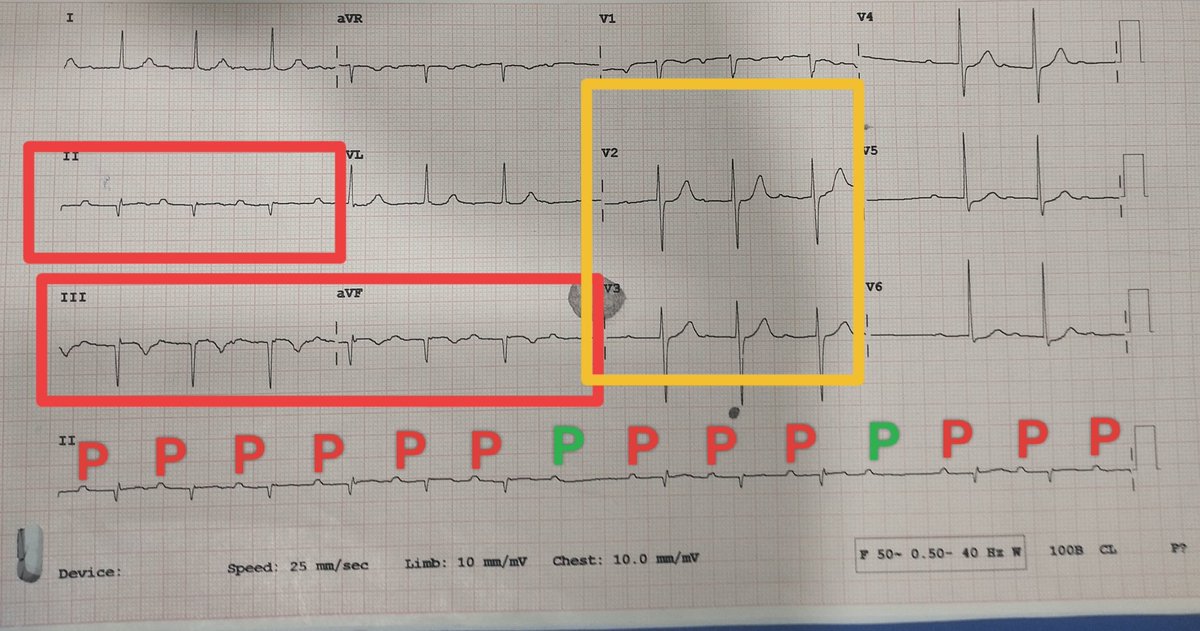
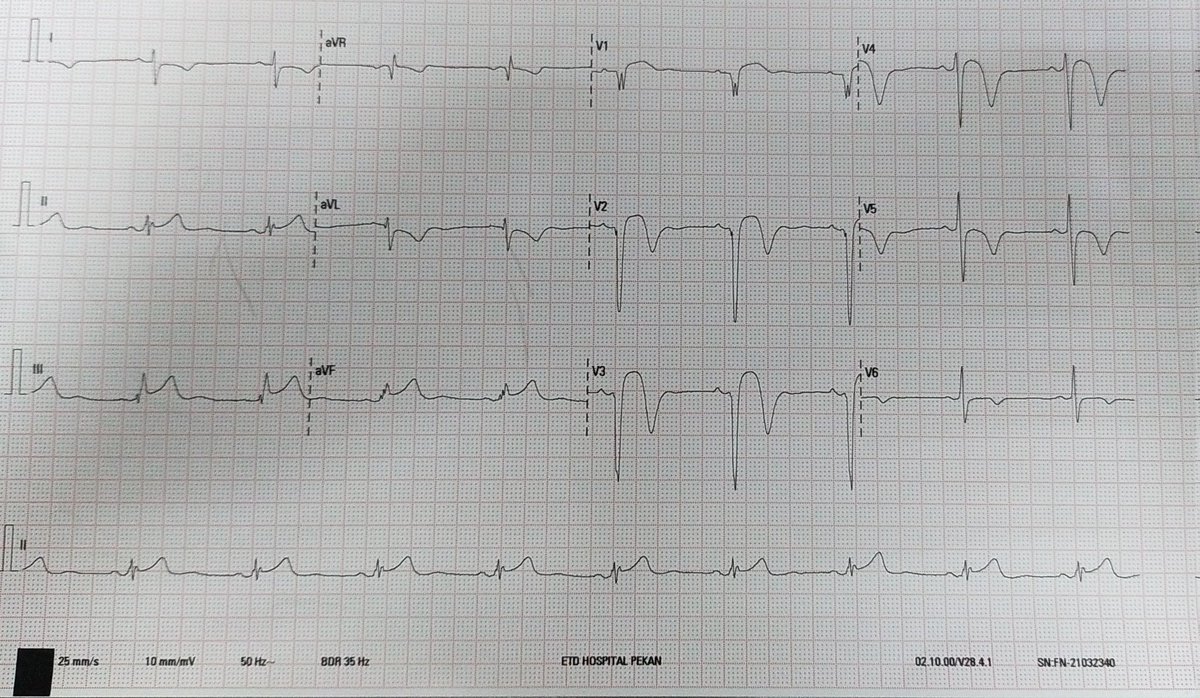
57 y/m farmer from Bangladesh presents with chest pain and syncope. Similar history 5 days back.
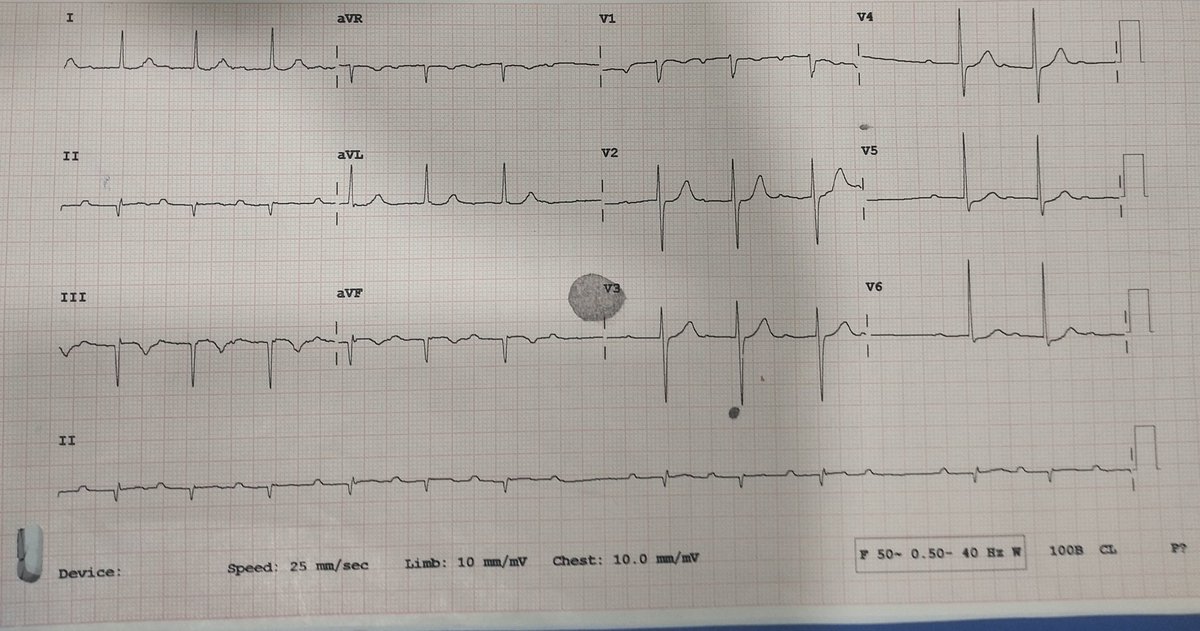
Here's the ECG.
Quantitative Trop T 2.09
What should be the next line of management?
@ecgandrhythmRoe@EcgsOnly@smithECGBlog@EcgOxford@DrRazi4
@EMBoardBombs Agree. Usually anterior leads is enough.
2 problems though.
A. When dealing with cardiologists, they are insistent on posterior ecg and
B. Exam curriculum still stresses on this
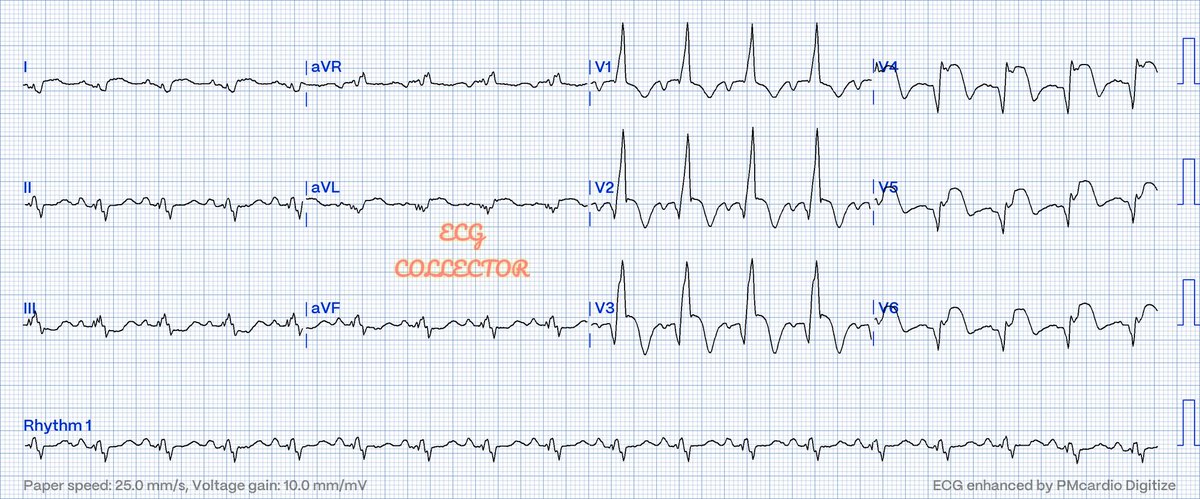
@The_Nanashi_O@DrRazi4@EM_RESUS@smithECGBlog@EcgsOnly My thoughts exactly. Because the reperfusion t waves seems too deep as compared to what i usually encountered and it extends beyond d lv aneurysm ecg changes at v2 v3
@mohda_nas@DrRazi4@EM_RESUS@smithECGBlog@EcgsOnly Wellens' syndrome, it seems.
Note that inferior TWs are not hyperacute — they are really reciprocal to reperfusion changes in the high lateral territory.
LAD occlusion with spontaneous reperfusion — needs urgent Cath.
@mohda_nas Nice ecg mate..cud thr be multiple culprits..hmmm
Inf and lateral has significant changes indicating Inf wall omi..meanwhile v2/v3 shows a biphasic...
Cud it be high lateral or wrap around LAD...
@DrRazi4@PMcardioBot Why the r wave is so large at v1-v3? It kinda looks like rbbbish with clear ste. In facility without pci, how "fresh" would u say this omi is? Because we know q wave is not reliable to say it is old infarct
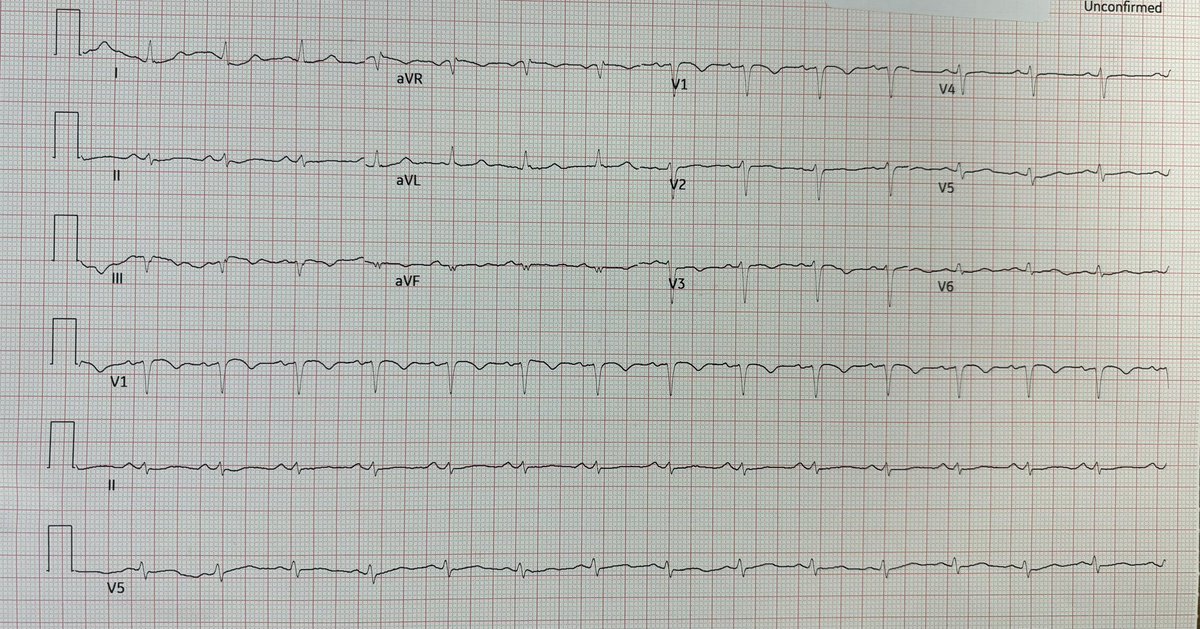
Case of silent ischaemia; old guy with poor Diabetic control; no chest pain at all; reduce effort tolerance for few days; stable VS; midzone crepitations; Trop T>2000ng/dL.
#ecg@PMcardioBot