
@AbiSivaMD @PathologyPat @muschollings Might help select I/o sensitive disease in this otherwise cold histology. Especially seeing mPIK3Ca enriched! Tissue based TMB still ideal. Nice correlative study!
English
Ankur Mehta
170 posts



CAPItello-291 PTEN analysis: NGS–IHC agreement: Overal 87.0% PPA 71.9% NPA 88.5% Among samples without PTEN alteration by NGS, 11.5% had PTEN loss by IHC. In the PTEN-deficient group, capivasertib + fulvestrant: mPFS 9.3 vs 3.7 months HR 0.52 In the NGS non-altered/unknown but IHC PTEN-deficient group: n=32 mPFS 16.2 vs 4.6 months HR 0.43 Relying only on NGS for PTEN may leave some patients out. IHC may identify additional candidates for capivasertib. aacrjournals.org/clincancerres/…


Didn’t Serena-6 show a >9 mo improvement in ESR1 mt 🤔@oncoalert #bcsm
In mBC, not all imaging changes mean your therapy has stopped working and switching too early is a real risk. 1/ RECIST 1.1 sets a clear bar for progression: ≥20% increase in the sum of target lesion diameters (with ≥5mm absolute increase), unequivocal progression of non-target lesions, or new lesions. Not every change on imaging meets this threshold. 2/ Three scenarios commonly and incorrectly flagged as progression: new asymptomatic sclerotic bone lesions, small mm asymptomatic changes in known lesions, and increased SUV on PET without corresponding size change. None of these, in isolation, trigger a therapy switch for me. 3/ Sclerotic bone lesions deserve particular attention. When effective therapy kills tumor cells in bone, the body lays down new bone matrix appearing dense and white on CT. This is a healing response, not new disease. 4/ The consequences of switching too early are real: loss of disease control from a working regimen, premature exhaustion of sequencing options. 5/ My approach: I integrate clinical symptoms, tumor markers, and serial scans together before making any decision to change therapy. 6/ Bottom line: confirm true progression before changing course. When in doubt, a short interval rescan is almost always preferable to an unnecessary switch. #BreastCancer #MedOnc


PATINA trial: maintenance palbociclib after first line anti-HER2+chemo in HER2/HR+ metastatic BC: - PFS benefit, no OS (not mature) - significantly more toxic (including financial) - significant early censoring imbalance (estimated 6% versus 12% over first 6 months in both arms, see Breaking-ICE App) -> makes PFS results less reliable, particularly in open-label trial - nonetheless the biological rationale, it is possible that ultimately no OS benefit will be seen "Adding toxicity without an improvement in clinical endpoints should generally be avoided." -> read our essay on PFS and other surrogates here : bmjoncology.bmj.com/content/3/1/e0… @vkprasadlab @VPrasadMDMPH


Thrilled to share results from the TACITO trial, just out in @NatureMedicine! FMT vs pbo in mRCC pts receiving pembrolizumab + axitinib. Look at the posts for more👇 @gianluca1aniro @ciccarese_c @DrChoueiri @montypal @tompowles1 @OncoAlert @KidneyCancer @urotoday @Unicatt
• Early TNBC: 74.3% •Non–high-risk HR+/HER2−: 91.2% ⚠️~60% of monarchE-eligible patients did not receive adjuvant abemaciclib Underuse most evident in N1 disease and older patients 📌 N1 ≠ Low risk N1 + Grade 3 or tumor ≥5 cm = true high-risk biology ET alone is insufficient

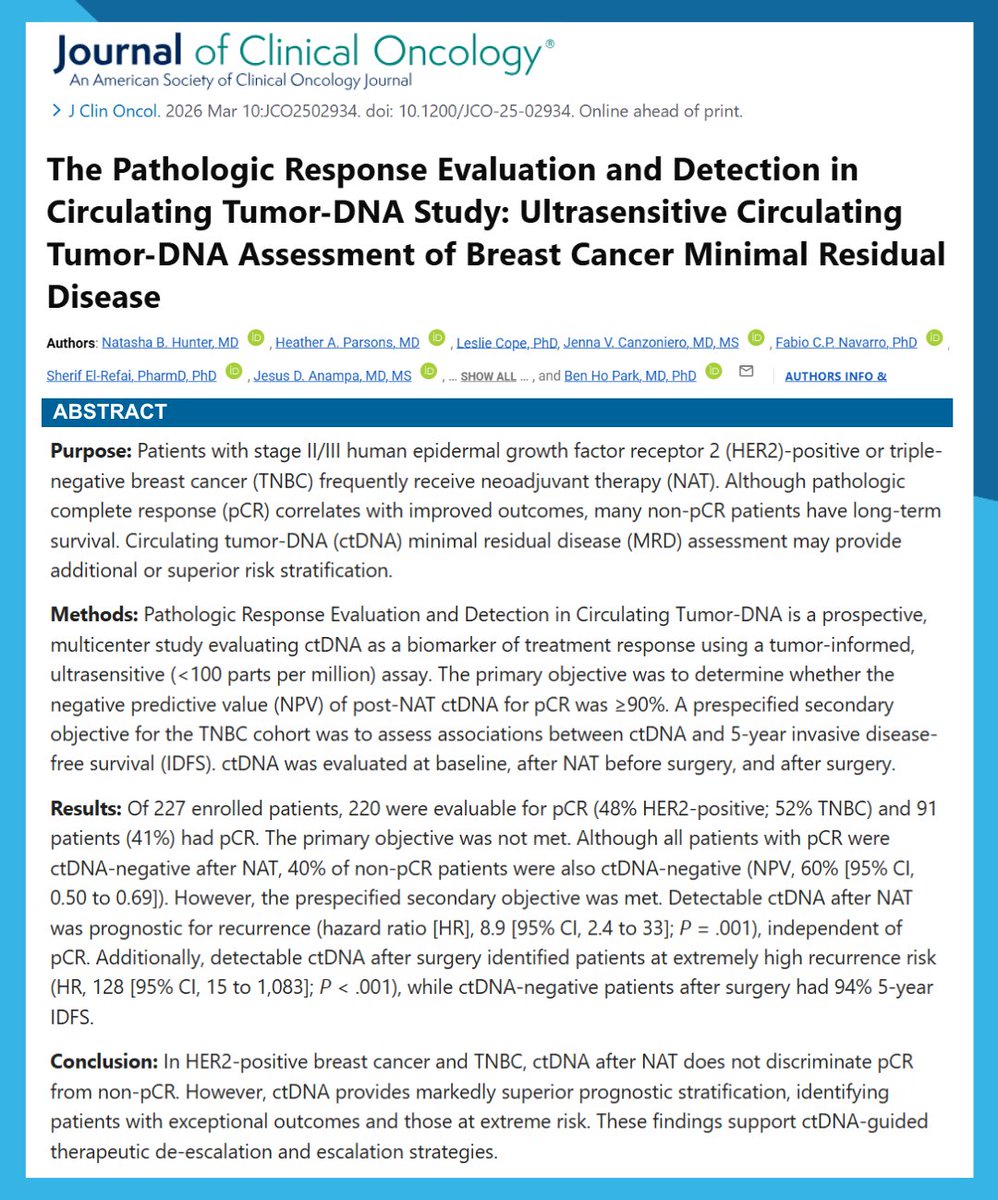
For a decade, the SoC for HER2+ eBC has been neoadjuvant TCHP. Yet, multiple signs suggest we may be moving towards a new SoC. A more tailored one. In this JCO editorial to NeoCARHP, I review the seismic shocks that are reshaping algorithms for HER2+ eBC. ascopubs.org/doi/10.1200/JC…


Trends in target novelty in oncology research and development Most late-stage oncology drugs are not truly targeting novel biology. Although more than half of targets are novel at the preclinical stage, this proportion drops to roughly one third by phase III. What ultimately reaches clinical practice represents only a small fraction of the initial biological innovation. First-in-class drugs are fewer in number but disproportionately influential. In 2024, 41% of global oncology revenue came from first-in-class agents, despite these drugs accounting for only 31% of marketed products. The therapies that meaningfully shift clinical practice tend to come from this group. The balance between modality and target reflects deliberate risk management. Novel targets are more often pursued using established drug platforms, whereas new technologies are preferentially tested against validated targets. This approach aims to contain clinical development risk. The ADC strategy is clear: innovation lies in architecture, not the target. Most ADCs do not introduce new biological targets; instead, they exploit proven targets such as HER2 and improve efficacy through payload and linker optimization. Clinical benefit is largely driven by this structural refinement. The ‘me-too’ race starts well before approval. Targets such as CD137, CD47, and CDK2 attract dozens of parallel clinical programs. High density in a target space does not necessarily equate to strong or differentiated clinical benefit. The TIGIT experience is instructive. The collective failure of multiple phase III TIGIT programs underscores that being a novel target alone does not guarantee clinical value. 💬True clinical breakthroughs often arise from genuinely new targets, but this path carries substantial risk. Much of the progress seen in daily practice instead comes from smarter and more effective ways of exploiting established targets. nature.com/articles/d4157…