🎉 Out now in the British Journal of Haematology 🙌🏽
⤵️ PTCy to 35 mg/kg improves platelet engraftment and ⤵️ bloodstream infections peri-transplant WITHOUT ⤴️ acute GvHD after MUD transplant 💪🏽
Team @pmcancercentre 🙌🏽
@BrJHaemshare.google/R7USoQ94Q3Go4h…
🚨 This is it people … you heard it first at #ASH25 🚨
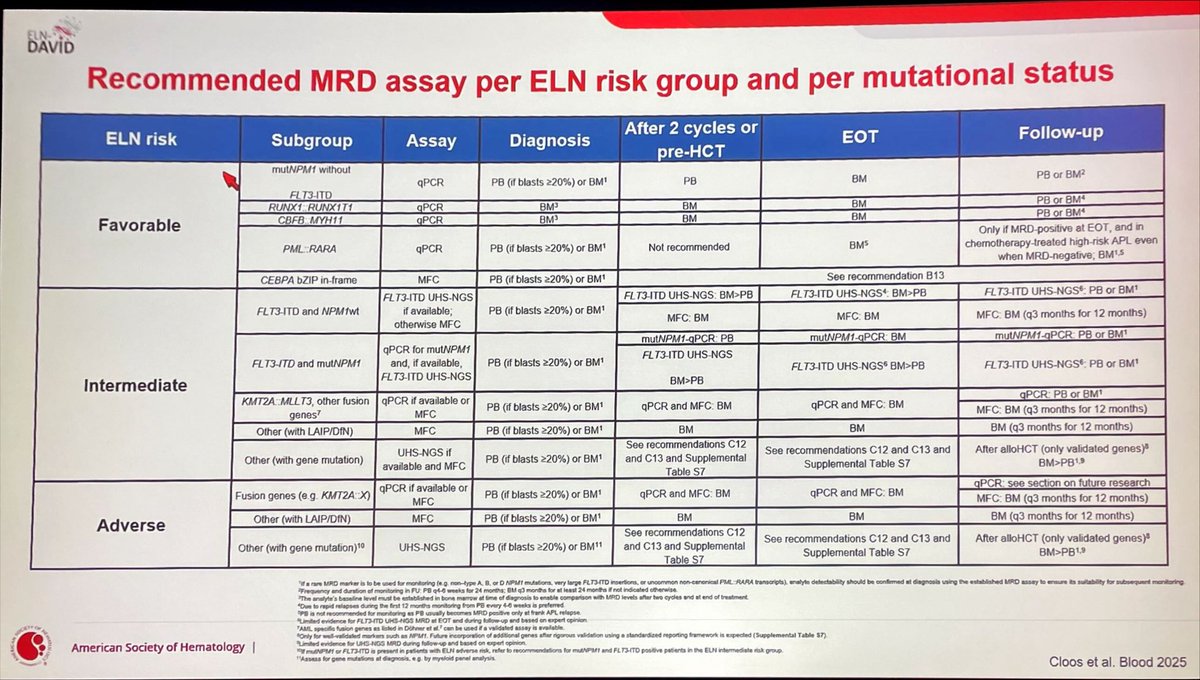
ELN #MRD 205 guidelines are in press in @BloodPortfolio
Bad news: It’s more complicated than before… 🤯
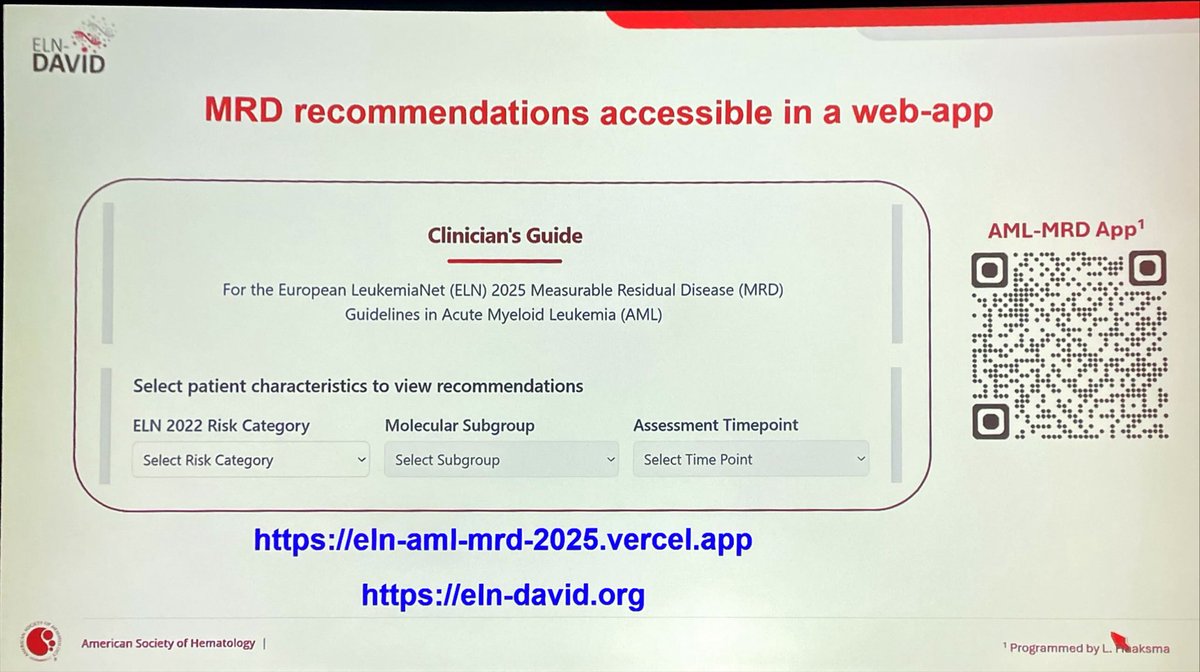
Good news: there’s an app for it 😉
eln-aml-mrd-2025.vercel.app
This article reviews current approaches to salvage #alloHCT for primary graft failure, highlighting a promising one-day conditioning strategy and the urgent need for standardized regimens to improve outcomes. astctjournal.org/article/S2666-…
AML-defining cytogenetic and molecular abnormalities (regardless of blast count)between the WHO 5th Edition (2022) and the International Consensus Classification (ICC 2022). #leusm#MedTwitter#hemonctrainees#when_on_service
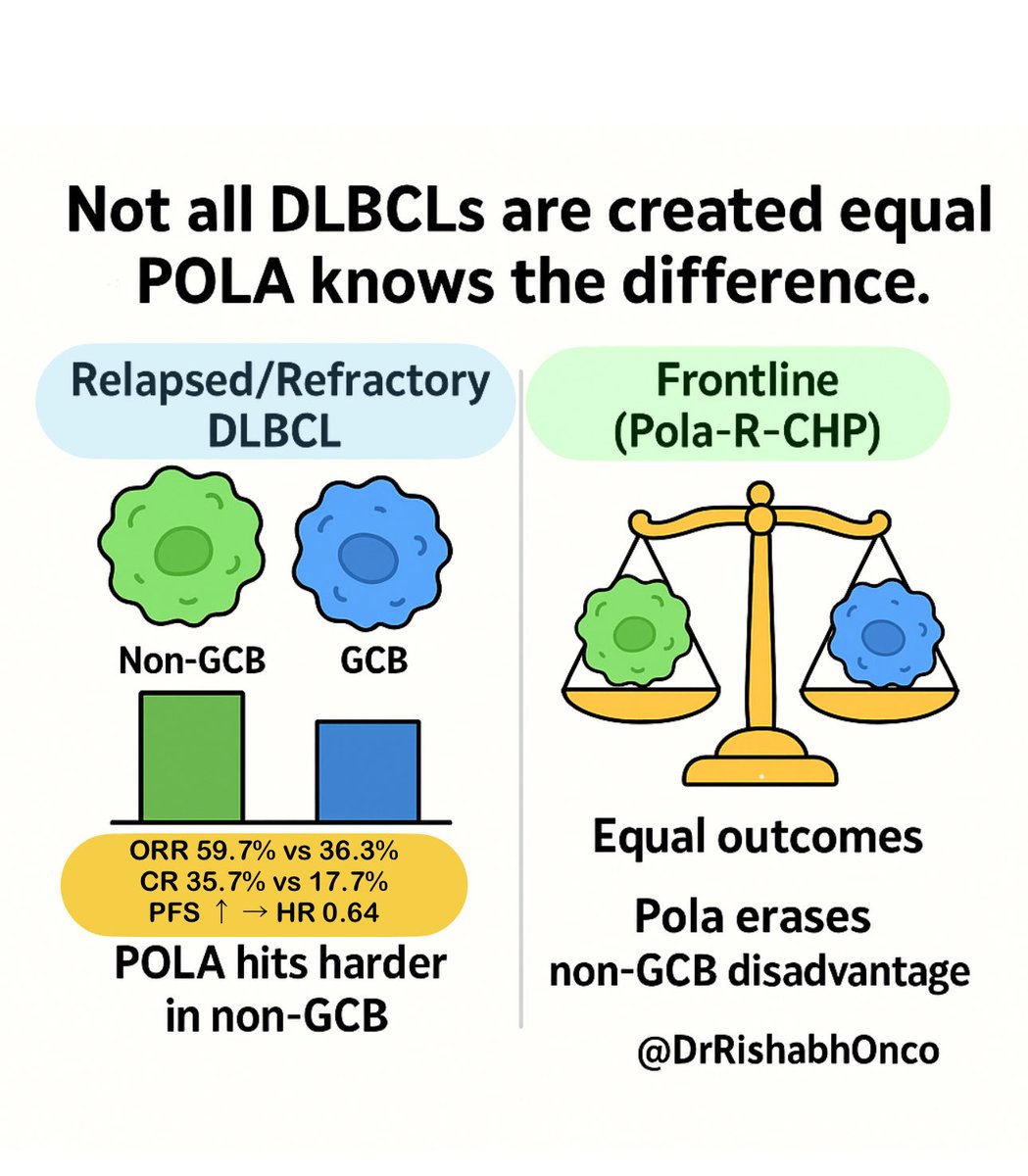
🧬 Not all DLBCLs are created equal - POLA knows the difference.
📊 Real-world (n = 740, 2015–24)
Polatuzumab used in
🔹Frontline (305)
🔹R/R (435)
COO classified by Hans IHC algorithm
🔥 R/R LBCL:
•ORR 59.7% vs 36.3% ➜ OR 2.6 (p<0.0001)
•CR 35.7% vs 17.7% ➜ OR 2.6 (p<0.0001)
•PFS benefit → HR 0.64 (p = 0.0006)
💊 Frontline (Pola-R-CHP):
No subtype gap → Pola neutralizes COO risk
💡 Takeaway:
Hans IHC still rules 🧪
🔹 Non-GCB = POLA favorite in R/R
🔹 Frontline Pola-R-CHP = great equalizer
📖 Scheffer-Cliff et al., Clin Cancer Res 2025
DOI: aacrjournals.org/clincancerres/…#DLBCL#Lymphoma#HemOnc#OncoTwitter#ESMOOpen@OncoAlert@esmo_open@ASCO
#Myeloma Paper of the Day: IFM2017-03 trial of Revlimid/Darzalex w/ 2 cycles of dex versus triplet w/ continuous dex finds DRAMATICALLY reduced progression risk (53.4 mos (95% CI 35.3-not reached) vs. 22.5 mos (HR 0.51, 95% CI 0.37-0.70, p<0.0001)): pubmed.ncbi.nlm.nih.gov/41038184/. #mmsm
What's going to be different with the new IMWG response criteria?
Main changes:
- FLC >=10 mg/dL with abnormal ratio takes precedence over urine (but urine is not gone)
- No more sCR
- Bone marrow to confirm CR can be performed +/- 6 weeks from blood testing.
- 24-hour urine at baseline, and if M-protein present, retest only to confirm CR
- Patients can be considered to have PD if they meet criteria by a variable not considered measurable at baseline (major weakness with current response criteria is that it misses light chain escape).
Next, imaging....
🧐Rarity in hematology🧐
Blastic Plasmacytoid Dendritic Cell Neoplasm (#BPDCN)
Rare but aggressive blood cancer with a name as complex as its behavior
Let's break it down in an educational🧵