Ron Levitin, MD retweetledi

We don't do 🧵threads too often, but we thought this Comments & Controversies piece is worth your 👀!
ascopubs.org/doi/10.1200/JC…
English
Ron Levitin, MD
990 posts

@rlevitinMD
Board Certified Radiation Oncologist at the Beaumont Health Lenox Outpatient Center in Southeast Michigan views my own














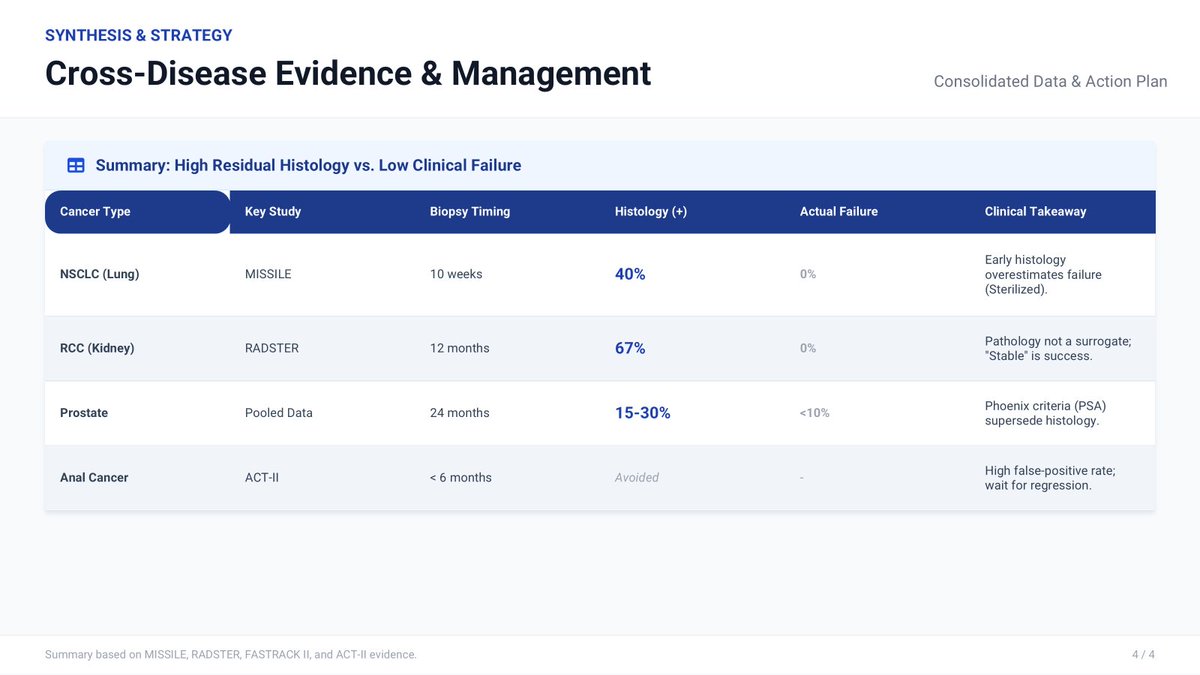
@jryckman3 @BrendonStilesMD @5_utr 100% agree. Just had a tough case (from a colleague)—post-SABR Bx showed ca without clear indication, and they rushed to surgery. Took a lot to convince them to hold off. MISSLE, RADSTER, ACT-II, and PSA were my go-to references as well.