Sabitlenmiş Tweet

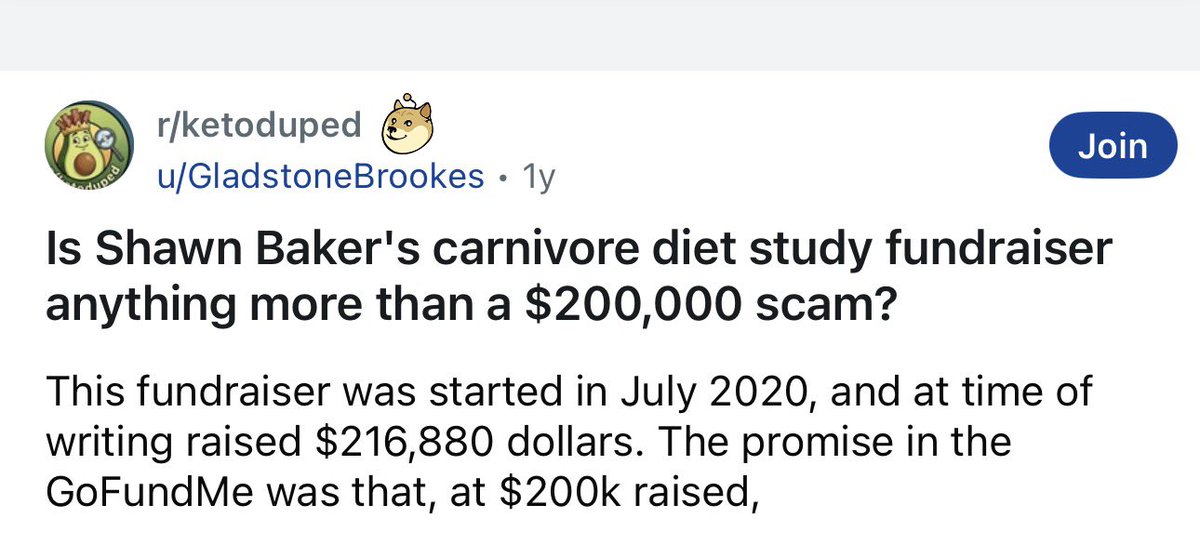
What happened to the clinical study that Shawn Baker was raising money for? Was that study conducted, or if not, where is the money?
English
Simon Hill MSc, BSc
18.5K posts

@theproof
Masters in Nutrition Science & Bachelor of Science (Physio). Author and podcast host. Science over hyperbole. Tweets are educational only, not medical advice.