Balázs Szigeti@psybalazs
🚨MAJOR NEW PAPER 🚨 just out in @JAMAPsych : Psychedelic Therapy vs Antidepressants for the Treatment of Depression Under Equal Unblinding Conditions (tinyurl.com/yu2rbtaf).
I am very proud of this one, was a lot of work for me - both co-first and last author! Eternal gratitude to co-first @QuantPsychiatry and twitterless Hannah Barnett!
The premise is that it is biased to compare open-label trials (=where patients know what treatment they are getting) to blind trials (=where patients do NOT know what they are getting). Open-label trials would gain an unfair advantage by higher placebo response. Even formally blinded psychedelic trials are practically open-label as its obvious to distinguish placebo from 25mg of #psilocybin. In contrast, traditional antidepressants (SSRIs/SNRIs) trials are are close to be truly blind (Lin 2022). Given the bias of open-label vs. blinded comparison, we compared the efficacy of psychedelic-therapy (which is practically always open-label) vs. open-label antidepressants for the treatment of major depression.
We tested 3 prior hypothesis:
- There will be a significant difference between psychedelic-therapy vs. open-label antidepressants, favoring psychedelic-therapy.
- There will be a significant difference between blinded and open-label antidepressants trials, favoring open-label.
- There will NOT be a significant difference between blinded and open-label psychedelic-therapy, as practically they are always open-label.
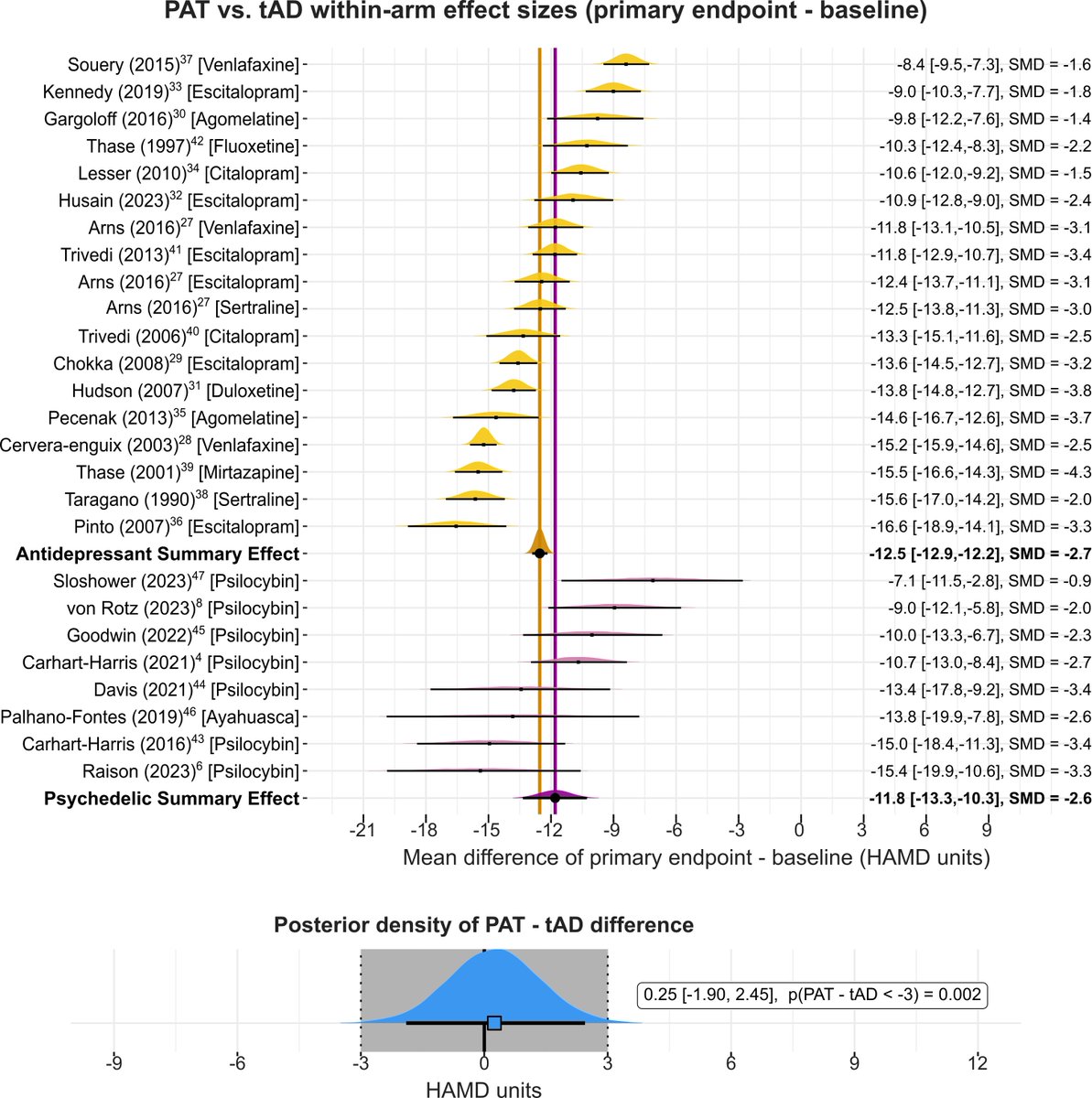
In contrast with our prior hypothesis, we did not find psychedelic-therapy to be more effective than open-label antidepressants (H1). Not only was the difference not clinically meaningful, but practically there was no difference at all. This finding means that antidepressants administered knowingly to patients, which is the case in real-life medical practice, is as effective as psychedelic-therapy. This result was robust across variations in study selection, including when we removed psychedelic-therapy trials on treatment-resistant depression.
We also assessed the impact of blinding in both psychedelic-therapy and antidepressants trials. We found that for antidepressants (H2), but not for psychedelic-therapy (H3), open label is associated with better outcomes than blinded treatment. However, even in the case of antidepressants, the difference was practically small (~1.3 HAMD units).
How come hypothesis 1 failed, i.e. that psychedelic-therapy is no ore effective than open-label antidepressants, given that antidepressants trials are famous for small drug-placebo difference (~2.4 HAMD units), while psychedelic-therapy trials reported large effects (~7.3)? The key factor is that in psychedelic trials the placebo response is about 50% relative to antidepressants, ~ 4 vs 8 HAMD units (Hsu 2024, Hieronymus 2025). This suppressed placebo response leads to an inflated between-arm difference, as the treatment arm is measured against a lower floor.
The suppressed placebo response in psychedelic-therapy trials is likely attributable to the ‘know-cebo’ effect, i.e. the disappointment when patients realize they are in the control group. In psychedelic-therapy trials, this placebo suppression accounts for 4.0 / 7.3 ~ 55% of the specific treatment effect. In other words, ~55% of psychedelic-therapy’s effect is not explained by patient improvement after the treatment, but rather by the lack of improvement in the placebo group.
In summary, we found that for the treatment of depression, psychedelic-therapy is no more effective than open-label SSRIs/SNRIs. Our results for psychedelics are twofold: psychedelic-therapy demonstrated a robust and large therapeutic effects (~12 HAMD units), which justifies optimism. On the other hand, psychedelic-therapy’s lack of superiority compared to open-label SSRIs/SNRIs highlights the influence of blinding integrity and argues against overly optimistic narrative's about psychedelic-therapy's potential.