پن کیا گیا ٹویٹ

Last few days for early bird! Join us in Montreal next september! #HR26 Nothing quite like it... thinkingcriticalcare.com/2026/01/16/fou…
English
Philippe Rola
23K posts

@ThinkingCC
#zentensivist, EMCrit Teammate, Proud daddy and husband. BJJ🟪. ICU Santa Cabrini Hospital.
What is the most reasonable immediate next step?

Kaiser LA wants to pay board-certified cardiologists $218.65/hr to work overnights and weekends. Don’t take this job. It’s hurts all of us.

📌 Surviving Sepsis Campaign 2026 Update (Key updates every RT & ICU doctor must know) 💀 What is Sepsis? Sepsis = life-threatening organ dysfunction due to infection 👉 In simple terms: Infection → Dysregulated host response → Organ failure #RespiratoryCare


🧠Utilización de la monitorización de la presión intracraneal no invasiva en pacientes con lesión cerebral⚡️ traumática tratada en entornos de bajos recursos: el estudio Intrigo🔰▪️Brasil Sergio. ▪️ Taccone Fabio S. 🧠El monitoreo de la PIC es un pilar en el manejo del traumatismo craneoencefálico (TCE). Sin embargo, en muchos entornos de bajos recursos: No hay disponibilidad de catéteres intraventriculares o sensores intraparenquimatosos😔 🧠Existe retraso en el diagnóstico de hipertensión intracraneal (HIC) 📚El estudio INTRIGO explora el uso de métodos no invasivos como alternativa pragmática. 🔍 Métodos no invasivos evaluados ▪️1. Diámetro de la vaina del nervio óptico (ONSD)👁 por ultrasonido ▪️2. Doppler transcraneal (TCD) Índice de pulsatilidad (PI)⚡️🧠 ▪️3. Evaluación clínica estructurada (GCS, pupilas)👁👁 💎 Perlas clínicas cafeteras ☕️ ✅ ONSD mostró buena correlación con sospecha clínica de HIC ✅ El índice de pulsatilidad (PI) se asoció con aumento de resistencia intracraneal ⚠️ Ningún método individual fue suficientemente preciso para reemplazar la monitorización invasiva ✅ La combinación multimodal (clínica + ONSD + TCD) mejoró la detección de HIC 🧠 La clave no es sustituir la PIC, sino aproximarse a la fisiología intracraneal mediante integración multimodal. 🧠Esto se alinea con conceptos modernos:Perfusión cerebral como objetivo central (CPP ≈ MAP – PIC estimada)⚡️🧠 💎Importancia de detectar pérdida de autorregulación cerebral ✅️Enfoque dinámico, no estático 🔴 1. La PIC no es un número, es un fenómeno fisiológico La hipertensión intracraneal es dinámica y multifactorial Los métodos no invasivos deben interpretarse en contexto clínico 🟠 2. ONSD:Umbral sugerido: >5–6 mm sugiere HIC ✅️Ventajas:Rápido, reproducible No depende de ventana ósea ⚠️Limitación:No permite seguimiento continuo preciso 🟡 3. TCD no mide PIC, mide fisiología cerebral ⬆️ IP elevado → ↑ resistencia cerebrovascular⚡️🧠 🧠Interpretación avanzada: ▪️IP alto + diástole baja → sugiere ↓ perfusión cerebral🧠 💎No confundir IP alto con PIC alta aislada‼️ 🔵 4. La integración multimodal es superior ▪️ONSD + TCD + clínica → mejor aproximación a HIC⚡️🧠 ▪️(ONSD ↑ + PI ↑ + deterioro neurológico = alta probabilidad de HIC) 🟣 5. Estrategia en entornos de bajos recursos. En ausencia de PIC invasiva: ⚫⚠️Evitar el error más frecuente‼️ ❌ Esperar signos tardíos (midriasis, herniación) ✔️ Actuar con datos indirectos tempranos🧠‼️ 👇🏽👇🏽👇🏽 Neurocrit Care doi.org/10.1007/s12028… https://criticalcarescience. 🔑🔒acrobat.adobe.com/id/urn:aaid:sc…
Who the f*** is that guy?






A man in Dubai suffered a sudden heart attack, within moments responders acted, using an advanced CPR machine to bring him back to life. 🇦🇪⛑️

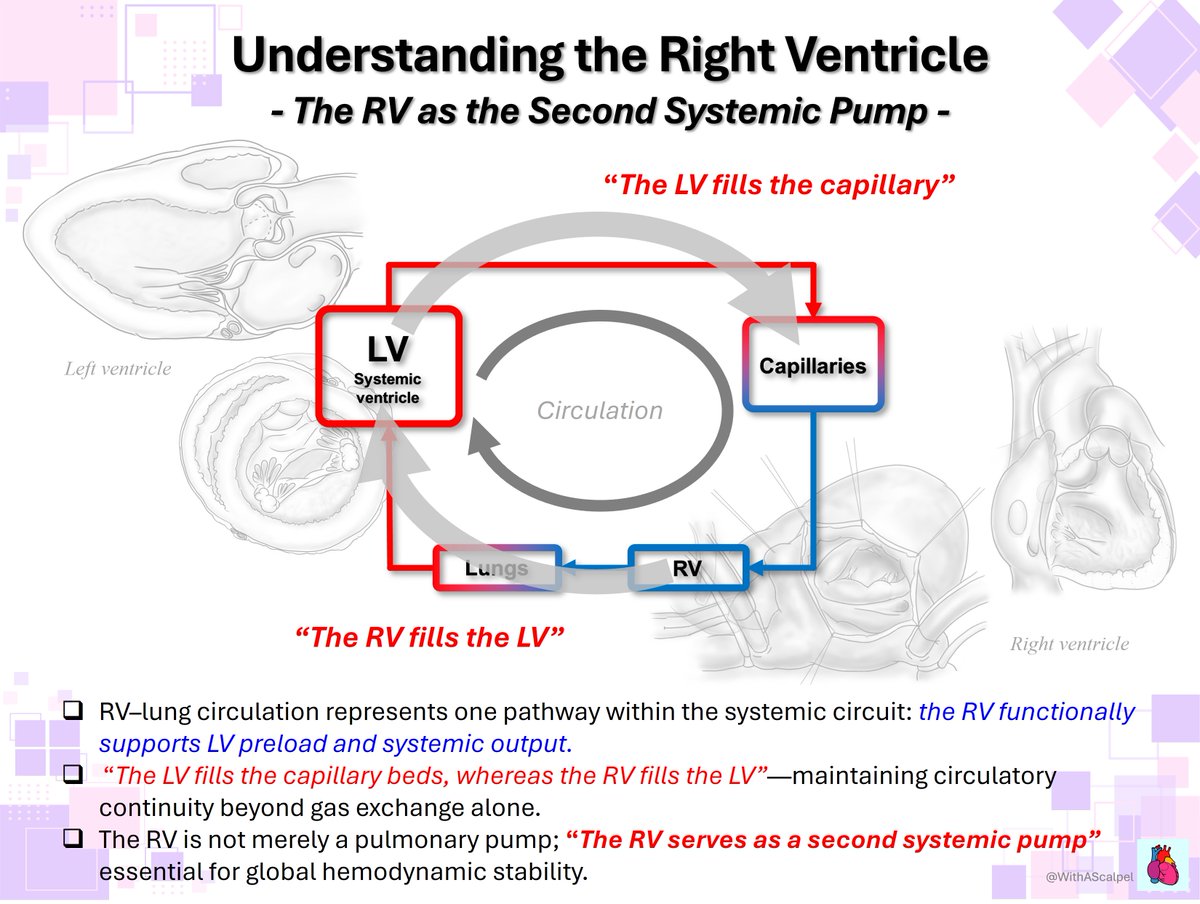
🫀The failing right ventricle: the most misunderstood chamber in critical care For years, we focused on the left ventricle. But in the ICU, the real killer is often the right ventricle. ->What is acute RV failure? 👉 Not just “weak contraction” It’s a hemodynamic collapse syndrome: RV dilation ↓ LV preload ↓ cardiac output ↑ venous congestion ➡️ → multi-organ failure ->The key pathophysiology (the vicious cycle) 1. ↑ Afterload (PE, ARDS, PH) 2. → RV dilation 3. → Septal shift → LV underfilling 4. → ↓ CO → hypotension 5. → ↓ RCA perfusion 6. → RV ischemia 👉 And the cycle accelerates ->The most important concept 👉 The RV does NOT tolerate pressure Handles preload very well Fails rapidly with afterload ➡️ Even small ↑ PVR → collapse ->Main causes you MUST think first 🔴 Pulmonary embolism 🔴 RV myocardial infarction 🔴 ARDS / mechanical ventilation 🔴 Decompensated pulmonary hypertension 🔴 Post-cardiac surgery ->Diagnosis is NOT obvious There is no single sign. 👉 It requires suspicion + integration: Clinical: congestion + hypoperfusion ECG + biomarkers POCUS (your best friend 🤓) Hemodynamics ->Echo mindset (fast ICU approach) 👉 Don’t overcomplicate Look for: ✔ RV dilation ✔ Septal shift (D-sign) ✔ TAPSE ↓ ✔ Venous congestion The real ICU mistake ❌ Treating RV failure like LV failure ->Management principles 👉 Think in 4 pillars: 1. Preload — “not too much, not too little” Hypovolemic → small fluid Congested → REMOVE fluid 👉 CVP is not a target, it’s a warning 2. Afterload, THE key target ✔ Treat PE ✔ Optimize ventilation ✔ Reduce PVR 👉 If afterload stays high → RV will fail 3. Contractility Dobutamine Milrinone Levosimendan 👉 Choose based on context 4. Perfusion pressure 👉 Norepinephrine is your anchor ✔ Maintains coronary perfusion ✔ Supports RV function ->Ventilation: the silent killer ⚠️ Positive pressure = ↑ PVR 👉 Over-ventilate → worsen RV failure ->When nothing works 👉 Think early: VA-ECMO RV assist devices 🤓Key insight This is NOT just a cardiac problem. 👉 It is a ventriculo–arterial coupling failure When: Ees / Ea ↓ → RV collapses 🤓Bottom line ✔ RV failure is preload dependent BUT afterload sensitive ✔ Small mistakes → rapid collapse ✔ Early recognition + physiology-based treatment saves lives ->Clinical mindset 👉 Don’t ask: “Is the RV failing?” 👉 Ask: “Why is the RV failing and, what is driving the afterload?” 📃Reference Giannakoulas G. et al. European Heart Journal (2025) 00, 1–16 doi.org/10.1093/eurhea…
