@DanielJDrucker @AppleHelix Its not clear if this is a true mechanism or if this is a PK effect. Probably the former IMO
English
Andy Jerome
841 posts
@jeromeinator89
Observations, one at a time - running and biopharma but mostly just killing time




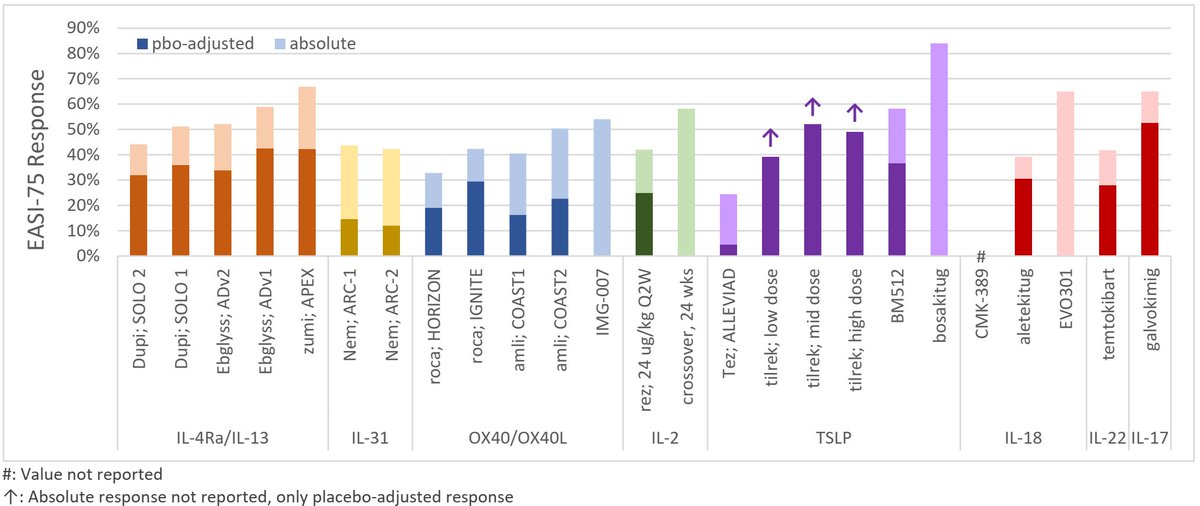


$APGE $xbi Good data for 777: APEX Part A data demonstrated durable maintenance of response at 52-weeks for every 3- and 6-months dosing, respectively, including: - 75% and 85% patients maintained EASI-75 - 86% and 78% patients maintained vIGA 0/1 Deepening of response was observed across all lesional and itch endpoints with both every 3- and 6- month dosing among the full population of patients initially randomized to zumilokibart Well tolerated across both dosing regimens, with safety profile generally in line with other agents in class.




This is absolutely inspiring! 81 years old, 29 sec 200m sprint!
Gov. Bob Ferguson says he'll sign the latest version of the Democrats' "millionaires tax." ebx.sh/4Sng9D

FUNDING: @TomColeOK04 says Pentagon is preparing to ask Congress for a supplemental $$$ bill to pay for Iran War
This is your heads up about the new scams that PBMs and their related companies are pulling. It is built on the following premise "Whoever controls care decisions controls revenue." The new "Rebate GPO" from PBMs is charging PEPM or PMPM fees to employers for "clinical services" . Can someone explain to me any scenario where a Pharmacy Benefit Manager would be the best source of clinical management services like the following : (PMPM) Specialty Drug Management $10 – $100 Coordination of specialty medications, utilization review, patient monitoring Digital Health / Remote Care Programs $20 – $40 Virtual care platforms, chronic disease apps, coaching programs Care Navigation Services $5 – $15 Member guidance, provider steering, benefits assistance Medication Adherence Programs $3 – $10 Outreach programs designed to improve prescription compliance Clinical Analytics & Employer Reporting $2 – $8 Data dashboards, utilization analysis, predictive modeling Prior Authorization Administration $1 – $5 Processing and management of prior authorization requests Biosimilar Conversion Programs $5 – $20 Drug switching initiatives and manufacturer coordination Outcomes / Value-Based Contract Administration $2 – $6 Tracking clinical outcomes tied to manufacturer agreements I'll say it again. The new PBM scam is to control care decisions WHOEVER CONTROLS CARE DECISIONS CONTROLS YOUR BENEFITS BUDGET. AND IT WONT BE YOU. IT WILL BE YOUR PBM You have been warned. @RepBuddyCarter @HawleyMO @SenWarren @RubenGallego @jamestalarico @SenSchumer @RFKJr_Official @modrnhealthcr @RosenthalHealth @chrisklomp @DrOz