
Ashok Krishnaswami
2K posts
Ashok Krishnaswami
@cardskrish
Boarded Geriatrics and Cardiology, #GeriatricCardiologist, Health outcomes, RCT. Clinician/Researcher, Aging advocacy, Views are my own. R/T != endorsement
San Jose, CA Se unió Mart 2010
929 Siguiendo839 Seguidores

This is not looking good for international delegates to ACC
I hope i make my connection in us!
Dr. Martha Gulati ♥️🫀❤️🩹🇨🇦@DrMarthaGulati
Hoping this gets better before departure day for #ACC26 but this is crazy at @iah #airport today No PreTSA open and 240 minute wait in the lines if what is posted is accurate. Please pay the TSA agents now. They need to pay rent, feed their families. Donations at food banks needed throughout Houston.
English
@DrIngold @drjohnm I'm forgetting the name of the exact epidemiological bias this refers to. But if we look at SAEs- something similar- no one blames the colonoscopy induced perforation that later passes away may weeks later in the ICU. @venkmurthy
English

Dr. Mandrola, correct me if I’m wrong here but isn’t that case just a massive error by the interventional cards doc for putting stents in an asymptomatic patient?
In the CAC—>Angio—>stents chain of events for an asymptomatic patient, the last thing to blame here is the CAC test.
Wouldn’t the correct application here have been PREVENT+CAC, and with CAC 710 w/o sx treat to secondary prevention target levels? I guess they could have also done SPECT and only revascularized if 10+% of LV ischemic maybe?
The trigger to angio and stent that patient isn’t the CAC test itself, it’s the fault of the Cardiologists for not doing their due diligence and taking into account the patient in front of them was asymptomatic.
English

Thank you Eric for sharing this story. It happens every day
Positive CAC leads to a search for ischemia which leads to angiogram and scant few docs can resist the urge. Your pt was lucky as it can even lead to bypass
Something needs to be done about this evidence-free practice
Eric Topol@EricTopol
@drjohnm I have been outspoken on the massive misuse of CAC testing for a long time (excerpt from my book in 2011) and have never ordered one.
English
English

@cardskrish @drjohnm @X @ihtanboga I'd say the tone on that blue place is far worse.
Meanwhile linked out is all just self promotion and mutual back slapping.
English
All those docs who left @x for that blue thing or link out basically were saying that political and in group signaling was more important to them than high quality commentary like this piece by @ihtanboga 👇
Anish Koka, MD@anish_koka
I don’t know folks… @x journal club is pretty top flight. Drug Coated Balloons non inferior to Drug Eluting Stents? Not so fast.
English
@DrMarthaGulati - as a noninvasive doc-loved his work-so sad to hear - 😢
English

Wow this is so sad to hear. Such a giant. Such a loss 💔
Elad Maor@maor_elad
Prof. @LermanAmir , a world authority on coronary microvascular dysfunction and my mentor at @MayoClinicCV , passed away today. He shaped my thinking as a physician and scientist, and I was fortunate to also call him a close friend. His scientific and human legacy will endure.
English
Ashok Krishnaswami retuiteado

Credit to my friend and mentor: @cardskrish
This picture is more than 14 years old with the pioneers of our field!
Proud to belong to this group of clinician scientists!
*Mark your calendars*
Our Annual Conference in Cardiovascular Aging will be hosted in the Heart House at American College of Cardiology in Washington, DC May 15-16, 2026: @venumenon10 @MichaelGNanna @tavrkapadia
Thanks for @ACCinTouch for supporting the field AND @ClevelandClinic for continuing the legacy!

English
English

Exciting to see @UTMBHealth launch a dedicated Geriatric Cardiology Fellowship 🧓❤️ One of the few programs nationwide, now expanding our training mission to 11 fellows/year—a major step forward 👏
@MShalabCardUTMB @ACCinTouch @DrDamluji #ACCGeriatric #ACCFIT #CardioTwitter
Mostafa Shalaby@MShalabCardUTMB
Excited to announce the new Geri Cards Fellowship at @UTMBHealth! 🩺❤️🧓 A 4-year integrated program (PGY4-7) offers:✅ Dual board eligibility✅Level II Imaging proficiency ✅ Research Start: July 2026. For more info and application: tinyurl.com/3xt5e87t
English
@DrJMarine Joe - Thank you for sharing! On another topic - Thank you so much for sharing your expertise for the CMP talks on EP topics. I learned a lot and helped greatly for continued ABIM certification!l🙏🏼
English

Patients have been asking me for many years why they developed atrial fibrillation. Great opportunity to talk about secondary prevention and mitigation. Some improved substantially with lifestyle changes alone. ahajournals.org/doi/pdf/10.116…
Seed Oil Disrespecter™️@SeedOilDsrspctr
Doctors are now openly mocking how patients are asking about the “Root Cause” of diseases instead of just taking the pills
English
Ashok Krishnaswami retuiteado
In collaboration with Dr. @MichaelGNanna @YaleCardiology, I am excited to launch the @ClevelandClinic Cardiovascular Center on Aging Grand Rounds & Distinguished Lecture Series
Sept 25, 5–6 PM ET, for the inaugural lecture by Dr. Daniel E Forman on aging & CV care. Open to all.

English
@gcfmd @HFSA @SJGreene_md @MKIttlesonMD @JavedButler1 @hvanspall @texhern @AndrewJSauer @dranulala @BiykemB @NMHheartdoc Thank you !
English

@cardskrish @HFSA @SJGreene_md @MKIttlesonMD @JavedButler1 @hvanspall @texhern @AndrewJSauer @dranulala @BiykemB @NMHheartdoc thelancet.com/journals/lance…
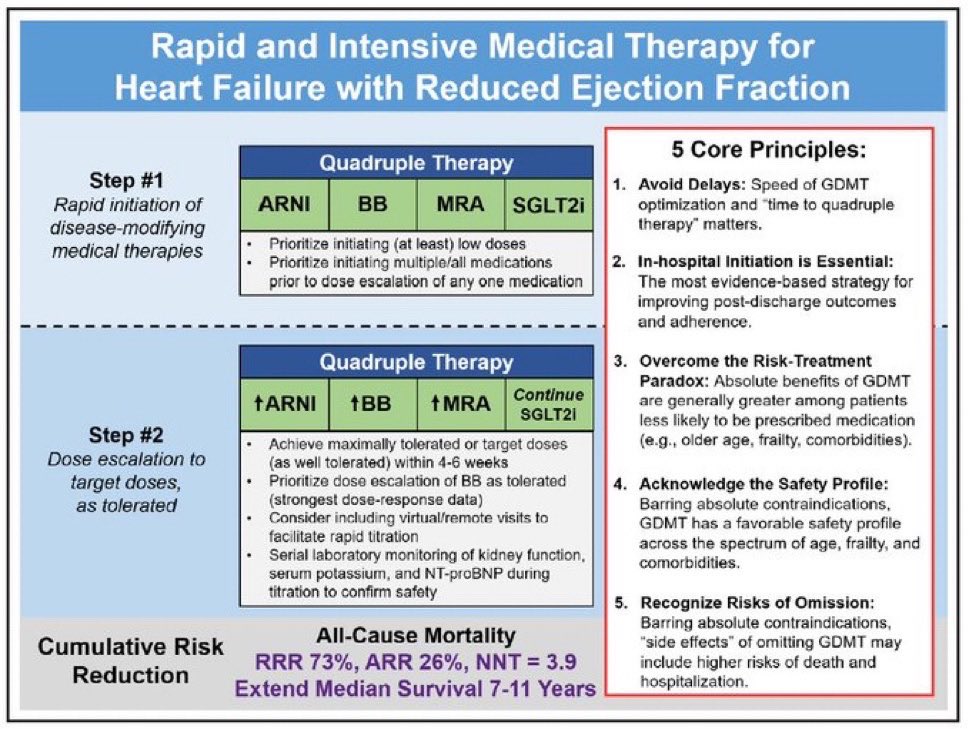
Along with other studies using restricted mean survival time (RMST) applied to RCTs of GDMT in HFrEF to estimate lifetime benefits
English
HFrEF
Q-GDMT (ARNI+BB+MRA+SGLT2i)
🛟 Extend median overall survival by 7-11 YEARS
Self-pay cash price all 4 💊
$121 per month
🎰 Incredible value
✅ Available now
What is your diagnosis to Q-GDMT time? ⏱️
English

For all of you who stop after the presentation: nothing is more true than the lesson in this image. So many abstracts are never published, and of those that are, the interpretation almost always changes, sometimes radically.
Elad Asher@AsherElad
Not mine, but I can't agree more... @PCRonline @Sbrugaletta @Ortega_Paz @Anazmicalik @guilbom @hect2701 @NicolaRyanI1 @DrPascalMeier @W_jyg @ICigalini @Hragy @SABOURETCardio @mmamas1973 @djc795 @GreggWStone @toreyj01 @EAPCIPresident @CMichaelGibson @SmithElliotjs @ArielRoguin @aayshacader @twj1974 #europcr @dangiloncardio @deharo_pierre @DanieleGiacoppo @MilasinD18
English
Great summary as usual my friend @DrDamluji . Agree with questions around not meeting PH assumptions. Would have been nice to see RMST analysis.
Abdulla A. Damluji, MD, PhD@DrDamluji
🥸2️⃣0️⃣ These findings highlight the need for caution when considering aspirin for primary prevention in older adults. In this population, long-term use *may* not be associated with cardiovascular benefit and bleeding risks remain a concern.
English
@cardskrish @DEF_gericard @MichaelGNanna @ParagGoyalMD @DrAROrkaby @minjikwak2 @GoalsDriveCare @AGSJournal @johnahartford @CircAHA @ACCinTouch @DrDaleNeedham @CircRes @VijayKunadian @KritiKalra092 @AmerGeriatrics @_WayneBatchelor @Yasserjamil_MD 🥸2️⃣1️⃣ Establishing cardiovascular centers on aging represents a transformative approach, meeting the needs of older adults with cardiovascular disease by bridging clinical care, research, and education, and creating a platform for the best possible health and quality of life!
English
Establishing Cardiovascular Centers on Aging: The @ClevelandClinic Experience: @JACCJournals
🥸 Very excited to report our work on CV Centers on #Aging
😱 With enormous support from @tavrkapadia @venumenon10 @LarsSvenssonMD @CandiceSilvers1
jacc.org/doi/epdf/10.10…
👇👇
English
@alexdeminaur stellar performance and gosh such a empathetic professional wining speech!🙏🏼
English
Ashok Krishnaswami retuiteado
Benefits of Cardiac Rehabilitation (CR): Mechanisms to Restore Function and Clinical Impact: @CircRes
🥸 Very proud of this work with my 2 mentors @DEF_gericard @DrDaleNeedham published in Circulation Research & @ParagGoyalMD
😱Molecular to Clinical Mechanisms of CR
👇👇

English
Ashok Krishnaswami retuiteado
🥸1️⃣ Cardiac rehabilitation (CR) reduces mortality, improves function, and enhances quality of life in cardiovascular disease. But <25% of eligible patients enroll, especially older adults, women, and those with frailty, disability, or limited access.
😱We need to do better.
English
Ashok Krishnaswami retuiteado
🥸2️⃣ CR targets three core physiologic impairments that drive exercise intolerance in CVD: low cardiac output, impaired vascular function, and dysfunctional skeletal muscle metabolism.
😱These mechanisms are interrelated and highly prevalent in older adults. (See Figure 1)

English
Ashok Krishnaswami retuiteado
🥸3️⃣ Stroke volume at peak exercise is often limited in CVD due to eccentric or concentric remodeling, ischemia, or impaired relaxation. All reduce cardiac reserve, impair contractility, and blunt VO₂ response; key contributors to frailty and poor outcomes.
😱(Look at Table)

English
Ashok Krishnaswami retuiteado
🥸4️⃣ Chronotropic incompetence is common in older patients. Age-related β-receptor downregulation and altered autonomic reflexes prevent heart rate from rising adequately during exertion, severely limiting cardiac output and exercise capacity.
English