AnnieC
270 posts


AnnieC
@CollierAnnie
Adopted a rescue dog, named him Nicky, but everyday would call out different names. He finally answered to a name - Batman! I adopted a superhero.

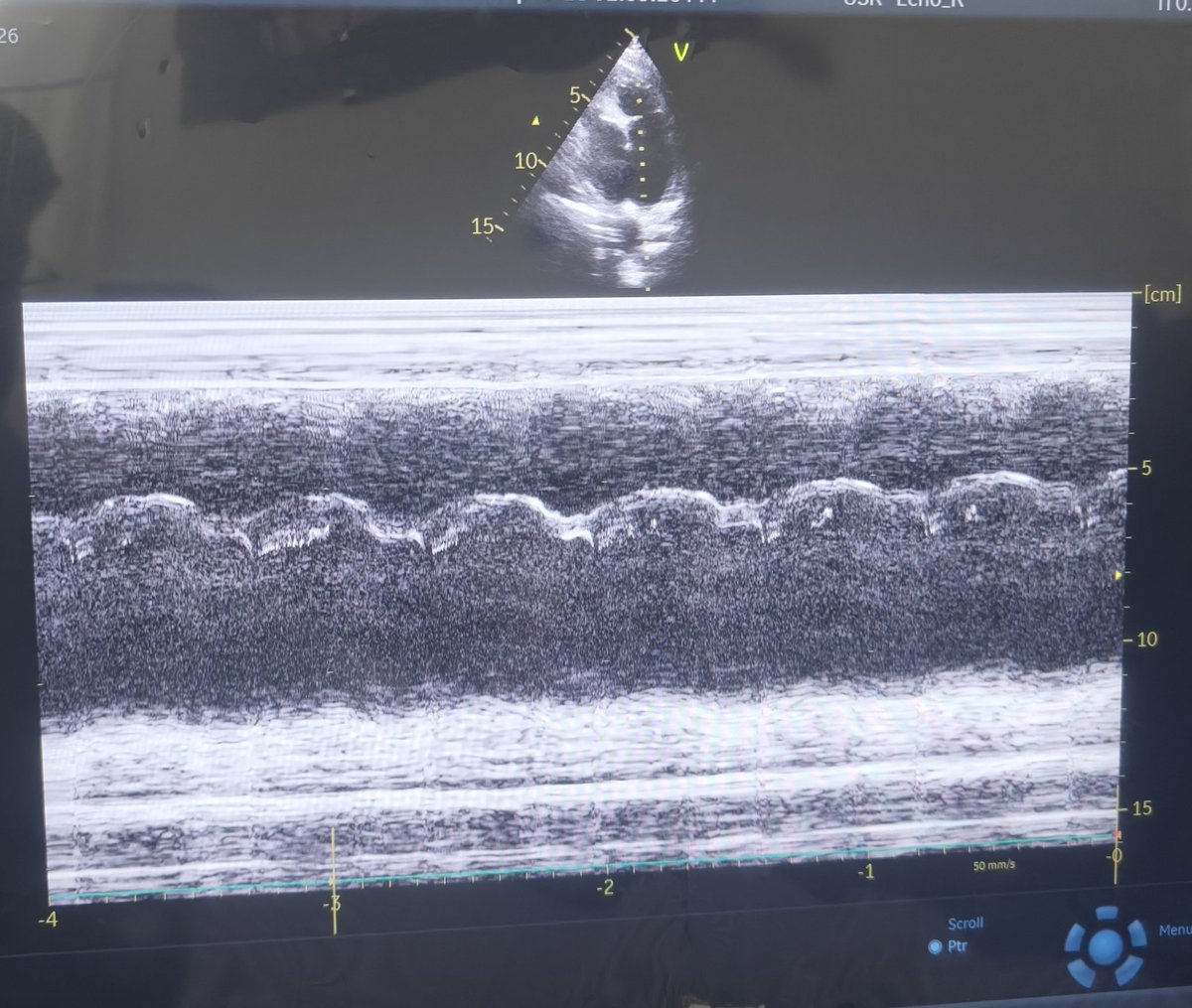


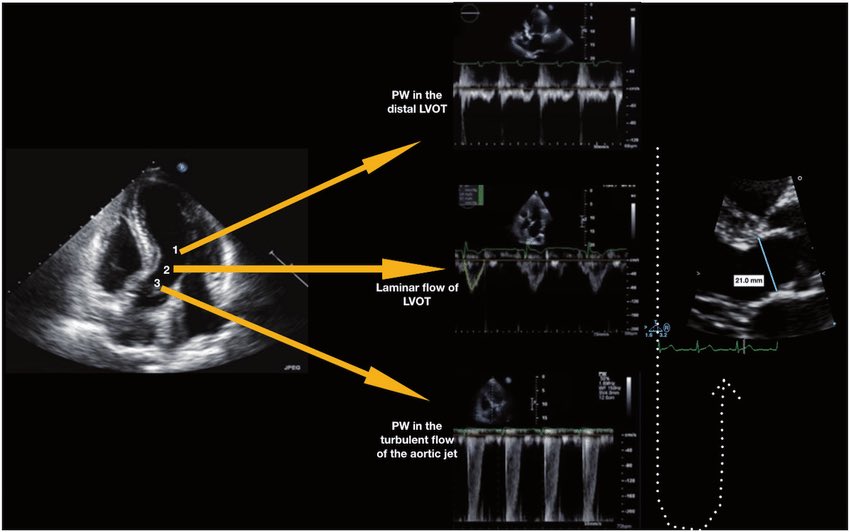











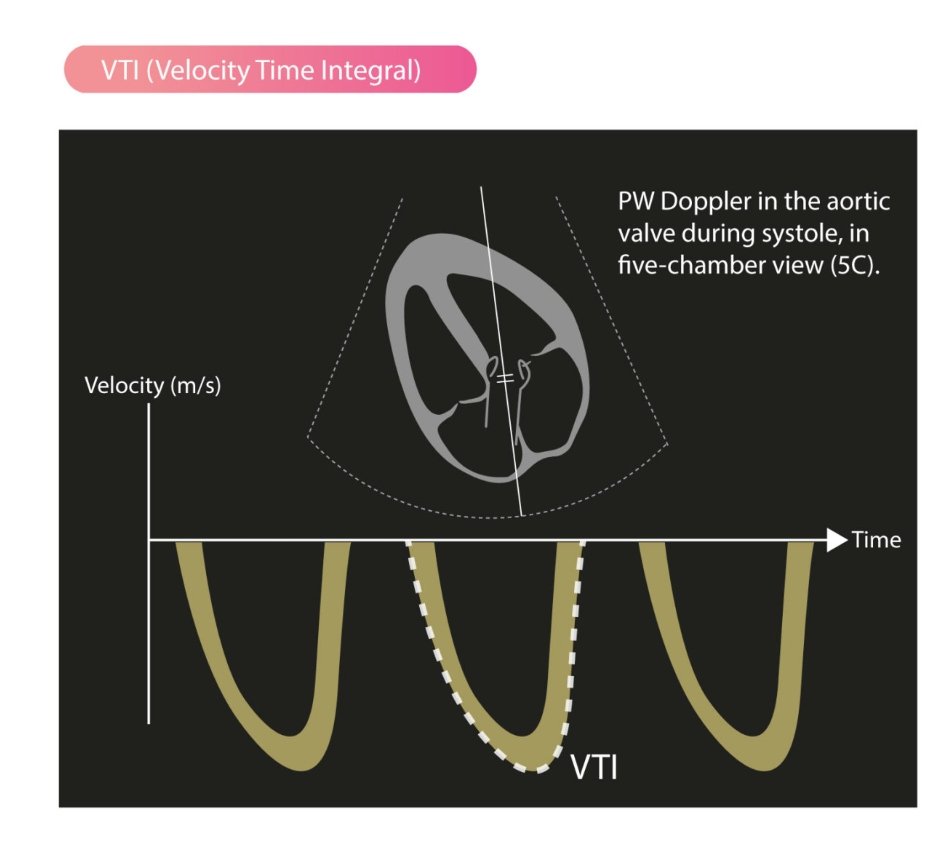



LVOT Vti: A Surrogate for Stroke Volume! 🔍 - Get a good PLAX view: Zoom in on the LVOT. - Measure LVOTd: Measure the LVOT diameter just proximal to the aortic valve at mid-systole. - Use PW Doppler: In A5C/A3C, place PW Doppler just proximal to the aortic valve. - Get a clean trace: Look for a clear Doppler signal with the aortic valve closing click. - Measure LVOT VTi: trace the modal velocity of the envelope! let the machine do the rest. This gives you an estimate of stroke volume! #POCUS #Shock #StrokeVolume #emergencymedicine #Scanuary Pitfalls : LVOTd measurement can be subject to error this will cause a big difference in your SV. So be careful!