
Dan Hess
28 posts

Dan Hess
@DHESS280
Heme/Onc Fellow at Duke by way of @universityofga, @UVaMSTP @lab_owens, @uabimres. Views are mine
Durham, NC Katılım Aralık 2021
117 Takip Edilen52 Takipçiler

@DHESS280 we have not yet used it as a routine- just in unique cases where my anxiety is high as to appropriate choice of therapy… i admit an expensive sleeping aid😉
English
The patient with a broken heart.
💔
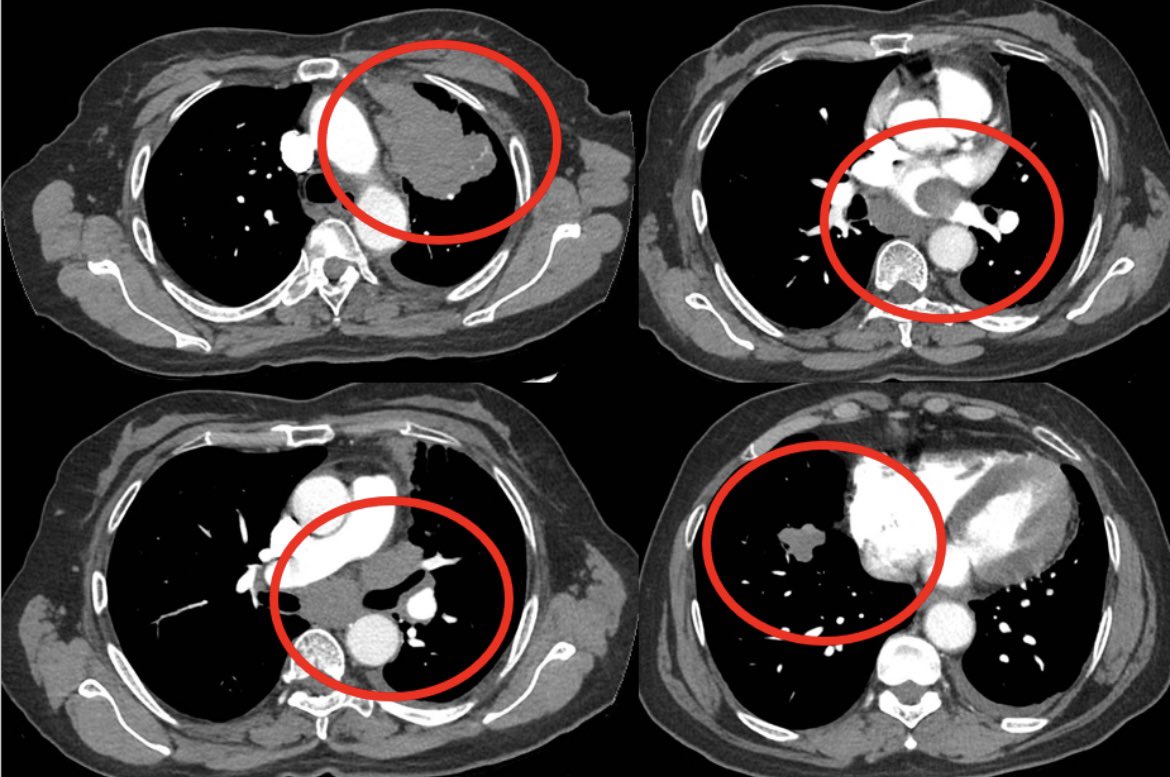
Pt in mid 60s with past smoking history presented with chest discomfort and dyspnea
Evaluation with CTA showed no PE but demonstrated a very large LUL mass with direct extension into mediastinum and L atrium and additional R sided lung lesions c/w st4 disease
Cardiac MR and ECHO confirm a mobile mass in L atrium contiguous w LUL mass
Path shows lung adenoca, PD-L1 TPS score >90%, ctDNA+ for K-Ras G12C
Tumor board review: surg/IR interventions not feasible, XRT likely not safe/effective, chemo - concern as to heme tox w heart invaded
Pt started on single agent IO

English
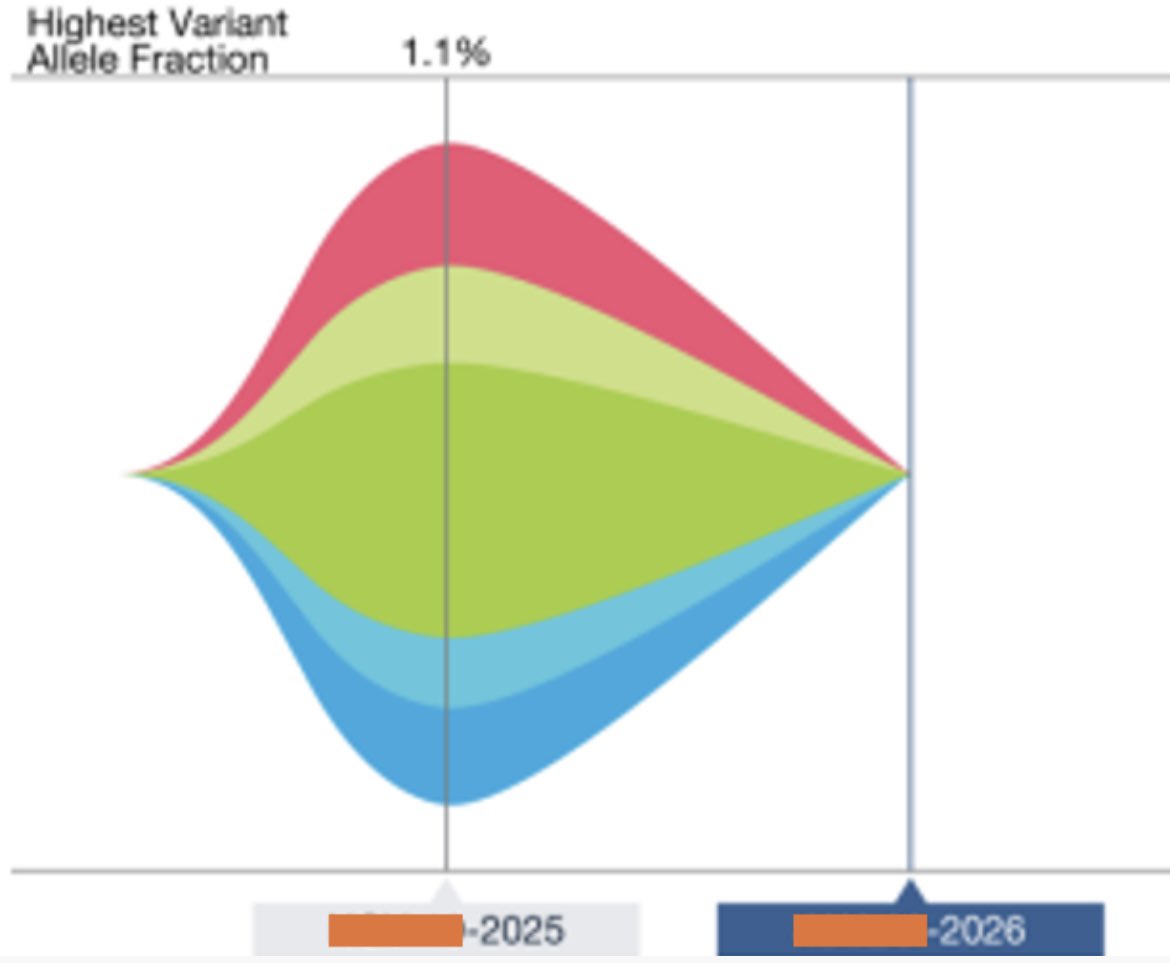
@BalazsHalmosMD Cool case, glad patient is doing well. Are you typically serially following ctdna in the metastatic setting like this?
English
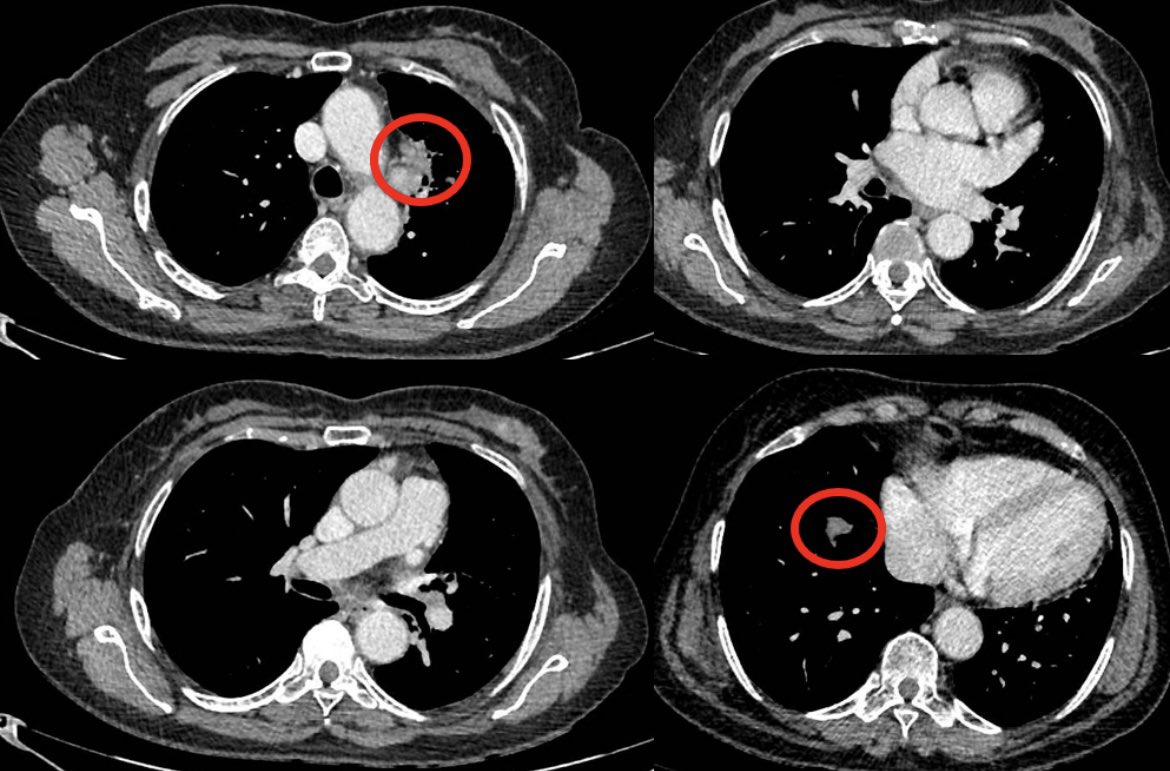
Patient has tolerated single agent IO well with limited eczematous derm AEs
Early ctDNA repeat showed clearance of ctDNA
Repeat imaging after 4 cycles demonstrated dramatic response to single agent IO w complete resolution of atrial/cardiac findings!
Guess it is good to have those hard-working T cells in circulation…
Heartfelt thanks to immunotherapy!!!
❤️❤️❤️
#lcsm
(W permission)
English
Let’s pause and think about what actually happens during a colonoscopy.
You’re sedated. A flexible tube with a small camera is inserted into the colon so physicians can examine the lining and remove abnormal growths at the discretion of the doctor. That lesion may become cancerous in 15-20 years or it may never become cancer. In the meantime, poking a little too hard with the instruments can make a hole, leaking fecal matter into your abdominal cavity. So you could end up with emergency surgery for a possible lesion that could possibly become cancerous someday.
Now, instead of reacting emotionally or projecting the program you’ve been given, step back and think logically. Does this sound like a good idea?
When a procedure can lead to death or permanent damage, don’t you think it’s time to rethink our approach?
English
Dan Hess retweetledi

Tailoring cancer care for older adults isn’t “extra” — it’s better care.
Proud of our team for showing that geriatric oncology can be implemented successfully in the community and meaningfully improve end-of-life outcomes:
Ramy Sedhom, MD, FASCO@ramsedhom
Proud to publish in @JCOOP_ASCO ascopubs.org/doi/full/10.12… Our design, implementation, & outcomes of our geriatric oncology program - emphasizing the role of health informatics & population health tools @PC3Innovation
English
@SuyogCancer We may have another option soon in camrelizumab + rivoceranib based on CARES-310 that was just published
English

So time for poll - what do u think is the first choice of option in your clinical practice for pt With metastatic HCC , fit ,child -Pugh A no comorbidities, no varices , with viral hepatitis , stable liver functions, access to all drugs .
Vote 👇 🗳 . Tell me why ?
English
@DrRishabhOnco Thanks for the reply and thanks for all the superb. I learn a ton from your posts!
English

🔥 HER2CLIMB-02: The systemic gain is small.
But the CNS gain? Hard to ignore.
🧪 Trial Design
Phase III, double-blind, 1:1
163 global sites
👥 Study Population
•Prior trastuzumab + taxane
•~89% prior pertuzumab
•44% brain mets (≈50% active)
•ECOG 0–1
💊 Trial Arms
•Tucatinib + T-DM1
•Placebo + T-DM1
📊 Primary Endpoint - PFS
⏱️ 9.5 vs 7.4 months
📉 HR 0.76 → 24% risk reduction
✔️ Benefit across ALL subgroups
🧠 Brain Mets Subgroup — The REAL Story
⏱️ 7.8 vs 5.7 months
📉 HR 0.64
🎯 Tucatinib once again shows disproportionate CNS impact
⚠️ Safety Snapshot
🔥 Grade ≥3 AEs: 69% vs 41%
🧪 ALT/AST ↑ (16.5% each)
🔄 Mostly reversible (median 22 days)
🚫 No new safety signals observed
💡 OS (Interim)
🕒 NR vs 38 months
📉 HR 1.23
⏳ Immature → more follow-up needed
🧭 Clinical Takeaway
Tucatinib + T-DM1 offers:
✔ Meaningful CNS protection
✔ Modest systemic PFS improvement
✔ Manageable hepatic toxicity
A relevant option when T-DXd isn’t accessible/suitable, especially in pts with brain mets 🧠✨
📖 Full paper in comment ⬇️
#OncoTwitter #BreastCancer #HER2 #MedTwitter @OncoAlert @myesmo @esmo_open @asco

English
Dan Hess retweetledi

ADCs: guided missiles, slow chemo infusion, or something else? In our latest free-access commentary, led by Matthew Vogel and just out in @JCO_ASCO, we review the latest evidence on ADCs’ mechanism of action, diving deep into their fascinating complexity. ascopubs.org/doi/10.1200/JC…

English
Dan Hess retweetledi

🔔Take a look at this article now published @NatureCancer !
'Tumor antigens preferentially derive from unmutated genomic sequences in #melanoma and non-small cell #lungcancer'
✏️By Pierre Thibault, Claude Perreault and colleagues
🔗nature.com/articles/s4301…
English
Dan Hess retweetledi

A commenter writes, "This makes my blood boil with anger."
Learn why he is right about a NIH funded study published in NEJM
sensible-med.com/p/a-new-costly…
English
Dan Hess retweetledi

I really don’t think people realize how incredibly hard and complex real cancer is to treat.
Oncologists would happily treat their dying patients with this.
It just isn’t true that there’s a simple off the shelf generic that magically cures all cancers.
Christina Brode@TeenaBrode
@anish_koka did your drug rep tell you that?
English
Dan Hess retweetledi

WELCOME: Dr. Matthew Hess to the Department of Orthopaedic Surgery! Hess is 1 of only 2 specialists trained in pediatric & adult orthopaedic surgical oncology in Alabama.
More: uab.edu/medicine/ortho…
@UABHeersink @uabmedicine @ONealCancerUAB @ChildrensAL @VABIRMINGHAM @UABNews

English
Dan Hess retweetledi
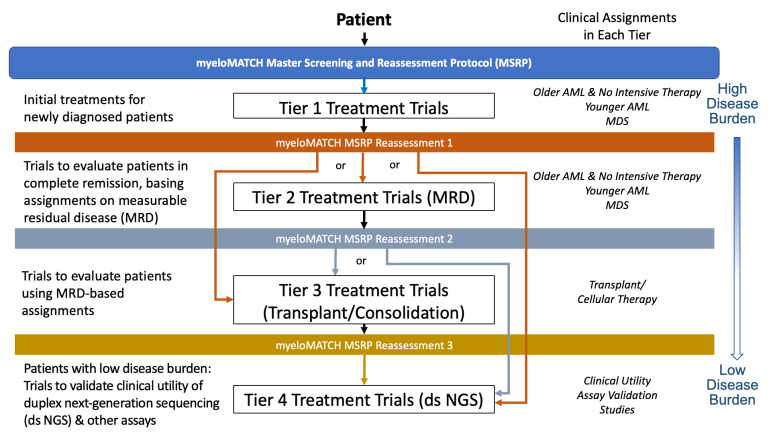
#myeloMATCH clinical trials are now open at @DukeCancer, using advanced biomarker testing to optimize therapy for patients with #AML & #MDS. An @theNCI precision medicine endeavor led by Duke's own Dr. #HarryErba and Dr. Richard Little of the NCI.
swog.org/myelomatch-ove…

English
Dan Hess retweetledi

A positive trial for cancer cachexia - a very distressing symptom to patients and caregivers! Congrats to my bud @MDRoeland for being an @NEJM author
Rami Manochakian MD, FASCO Cancer Education@RManochakian
🔥🚨@OncoAlert Hot off the press. Just published @NEJM in conjunction with presentation @myESMO #ESMO24 Results of #Positive Phase 2 trial of #Ponsegromab (#GDF15 inhibitor) vs #Placebo for treatment of #Cachexia in patients with #Cancer. 👇🏼 nejm.org/doi/full/10.10…
English

👏 Join us in congratulating our members who earned the Fellows of ASCO (FASCO) distinction this quarter! We're grateful for their extraordinary volunteer service, dedication, and commitment to ASCO. Learn more about FASCO distinction: brnw.ch/21wLvZf


English
Dan Hess retweetledi
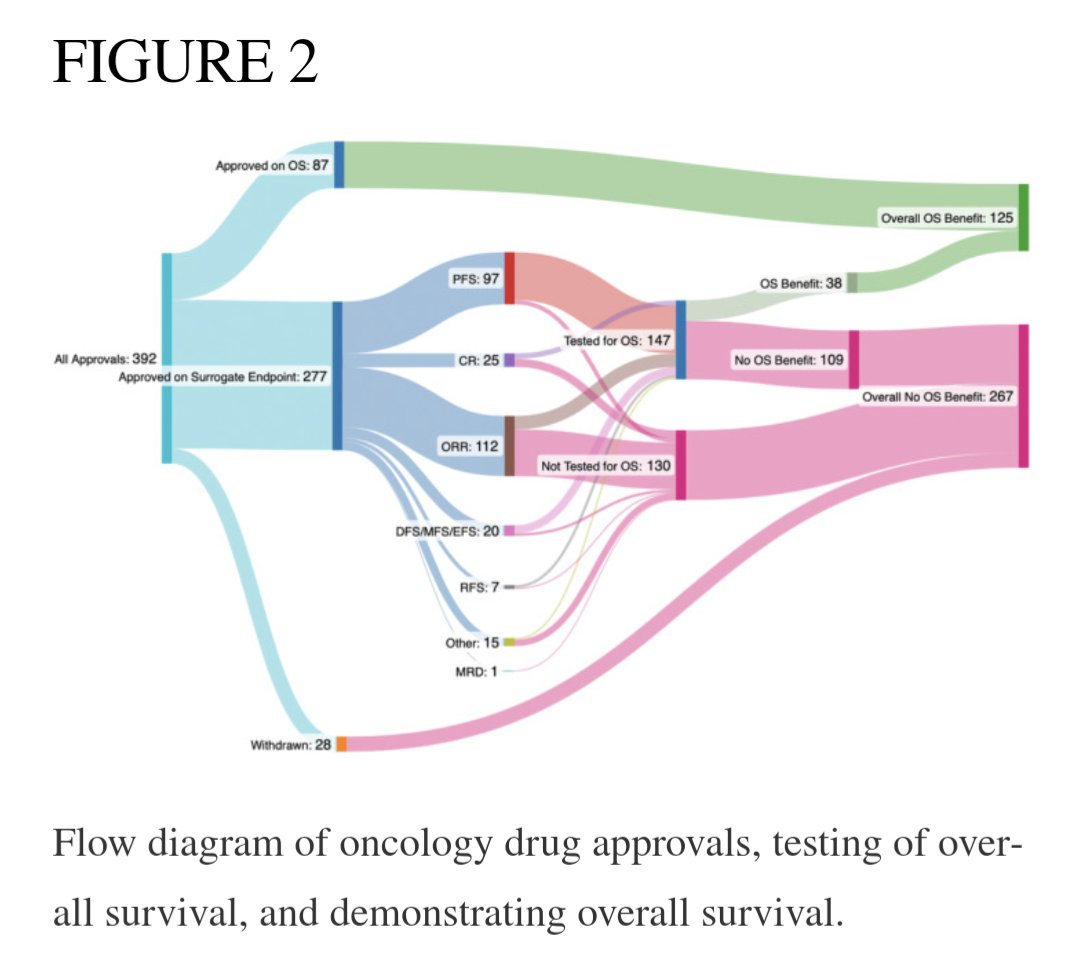
Less than half of cancer drugs approved based on a surrogate endpoint are ever found to improve survival in their entire lifecycle.
ncbi.nlm.nih.gov/pmc/articles/P…
English
Dan Hess retweetledi

An Interview with the Nature editor who rejected the paper that won the Nobel Prize
In mid-2000s, Katalin Karikó submitted one of her papers to Nature, the prestigious academic journal.
Nature desk rejected her paper saying that it did not offer any original insights and that Karikó’s work only makes an “incremental” contribution to the field.
The paper was later published in another academic journal Immunity and eventually became the basis for Karikó’s work that won her the Nobel Prize in physiology.
I tracked down the Nature editor who desk rejected Karikó’s paper and asked how he felt about Karikó winning the Nobel Prize.
Following is an excerpt of my conversation with the Nature editor who spoke to me on the condition of anonymity.
The conversation has been edited for mockery and ridicule.
Mushtaq Bilal (MB): Good afternoon! I hope it’s not too awkward a moment for you.
Nature Editor (NE): Just another day in the life of a journal editor who rejected potentially Nobel Prize winning work.
MB: How do you feel about being the editor who rejected that paper? Did you ever think something like this might happen?
NE: Oh Absolutely! I have a sixth sense for these things. I can spot a Nobel Prize winning paper from a mile away…and then reject it.
MB: Good to know you still have a sense of humor…
NE: …and a bit of false pride too.
MB: Have you considered adding it to your CV, “Professional Rejector of Groundbreaking Work?”
NE: That’s a good one. I am thinking of starting a new journal called “Nature Rejected” in which I will publish every paper rejected by Nature.
MB: Sounds like a best-seller to me…
NE: I could’ve been the editor who published the Nobel Prize winning work, I could’ve become the next star in academia. Nobel Prize winning scientist would mention my in their speeches, invite me to go to Sweden with them where I would get myself nice, relaxing Swedish massages…that’s my biggest regret, Mushtaq. I was so looking forward to those massages.
MB: I think we are getting off track a bit. Coming back to the paper, walk us through the day you rejected that paper.
NE: It was just another day. I woke up, applied for a few non-academic jobs, dropped my kids at school, fought with my wife over wet towels, had lunch followed by a huge relaxing fart, and then I rejected the paper.
MB: Some details are a bit unnecessary but let’s not get off topic again. Have to thought of sending a congratulatory message to Karikó? Maybe a fruit basket with a “My bad” card?
NE: That would be the class thing to do. I’m thinking of sending her a telescope. So, the next time she spots something groundbreaking, she can magnify it enough for even me to see.
MB: That makes no sense…
NE: I know. It’s a shit joke…
MB: It’s actually quite refreshing to see someone like you who owns up to their mistakes.
NE: Thanks. And please send me the transcript of this interview so I could take a look at it before you post?
MB: Why, you want to reject it too?
English
Dan Hess retweetledi
Our prospective study showing body composition differences among NH Black and NH white patients with GI cancer. @GrantWilliamsMD @smith__giri @DHESS280 @MFowlerPhD
authors.elsevier.com/a/1iniY6hK%7E0…
English