Sabitlenmiş Tweet

[INTRO TO PEPTIDES SERIES]
What is Peptide Therapy
(And How Does it Work?)
🧬 🔬 🧬 🔬 🧬 🔬 🧬 🔬 🧬 🔬
Peptide Therapy:
An Emerging Science
🧬 💉 🧬 💉 🧬 💉 🧬 💉 🧬 💉
THREAD 👇
English
Denis, NP 💉 Lifestyle Design
4.3K posts

@Denis_protocol
Your Protocol: Live in Your Sweet Spot, I'll show you how | Hormones, Nutrition, Fitness, Peptides, Sleep, Sex, Stress | P.S. Your 'Guru'? My Patient.




@AbudBakri Excited about your online clinic launch. I hope soon is really soon :)

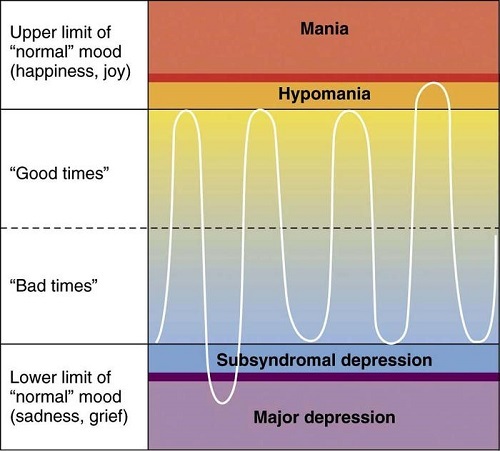
Microdosing fruit throughout the day will give you smoother, steadier energy than any nootropic. Mimics the effects of fasting without the manic feeling or crash. Spares protein (muscle) breakdown too. An apple an hour gives you great power





Maybe if you had sufficient androgens and insulin sensitivity, you wouldn’t need to be eating so much protein just to look like you kinda lift Both of those factors start in the mitochondria
Just like you can too little or too much of certain macros (carbs, protein, fats), you can get too little or too much of certain wavelengths of light (visible, infrared, UV) - Infrared is like protein, most don’t get enough - Visible (blue) is like carbs, most get too much and the low quality - UV is like fats, often demonized, but it is the wrong fat in the wrong context that is bad, just like UV Not perfect metaphor but you get the point