
SEMily, Char.D.
358 posts
SEMily, Char.D.
@Emily_EMPharm
EM pharmacy, healthcare simulation, toxicology, micro dose pressors safety, EM quality and safety, CritCare in ED, harm reduction. Animal lover. Views are mine
Earth Katılım Ağustos 2022
1.5K Takip Edilen666 Takipçiler
Large doses cause an extended duration of action and greatly increase risk of awareness with paralysis. If you haven’t read the ED-AWARENESS Study, please do so.
Rocuronium should be dosed at 1 mg/kg IBW (roc is hydrophilic) with the rare crash airway exception.
English
Rocuronium has a dose-dependent onset AND duration. While it is appropriate to give a dose at the higher end of the range for faster onset (up to 1.6 mg/kg IBW) in the setting of a crash airway, the practice of “blanket dosing” 100 mg for all patients should be reconsidered.
English


@PharmacyAcute This is excellent! Consider adding epinephrine potentially causing lactic acid elevation by increasing glycolysis and anaerobic metabolism. Can cloud the picture in post-arrest resuscitation!
English

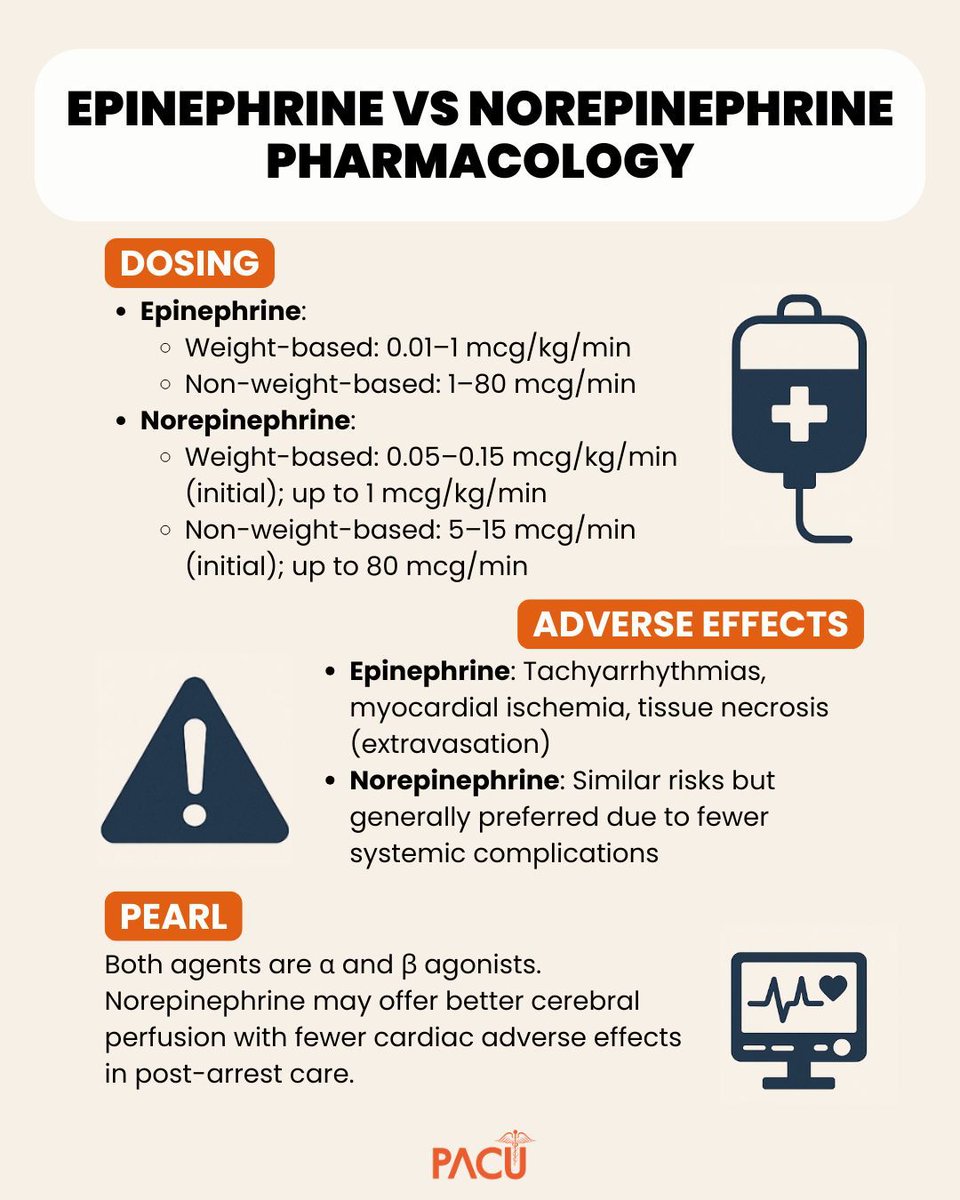
💉 Norepinephrine vs Epinephrine — Know the Difference.
From dosing ranges to key adverse effects and clinical considerations, understanding these vasopressors is critical in post-cardiac arrest care.
Save this for quick reference and keep it ready when seconds matter.
📚 See the full Pharmacy Pearl: pharmacyacute.com/pharmacy-frida…
#PharmacyPearls #PharmacyEducation #ClinicalPharmacy #CriticalCarePharmacy #EmergencyMedicine #PostCardiacArrest #MedEd #PharmacistLife #MedicationSafety
English

@IM_Crit_ Create a mechanism for experienced emergency, critical care, hospitalist nurse practitioners & PAs as well as CRNAs to advance into a physician role specifically through a very well regulated but distance solution and you could solve a huge part of the physician shortage
English

@PharmD_intheED Also, why no cath after? Thrombolytics are not a contraindication
English

SEMily, Char.D. retweetledi
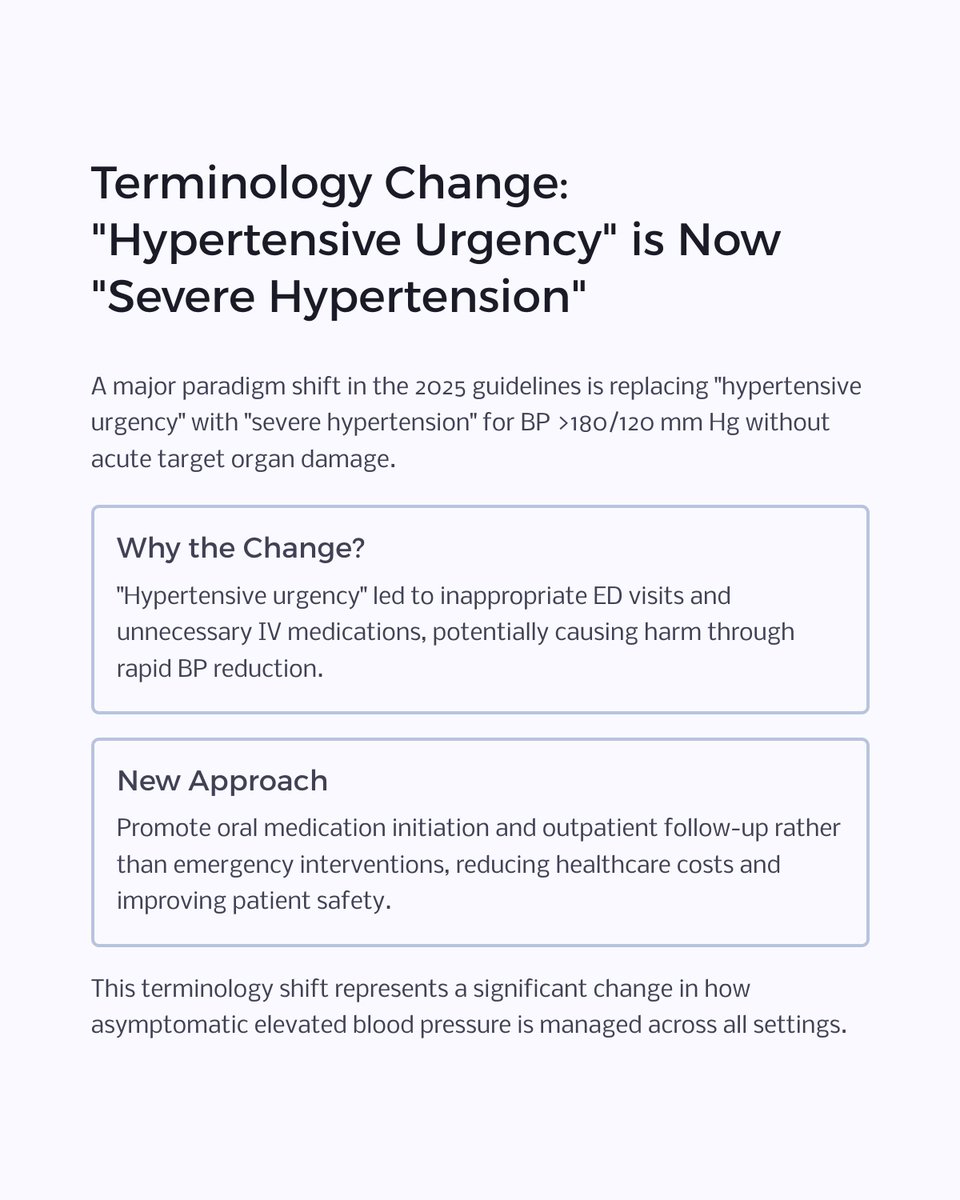
The 2025 AHA/ACC Hypertension Guidelines are out, and the changes are significant. Here are the key takeaways for pharmacists & clinicians:
"Hypertensive Urgency" is now "Severe Hypertension" for BP >180/120 w/o target organ damage.
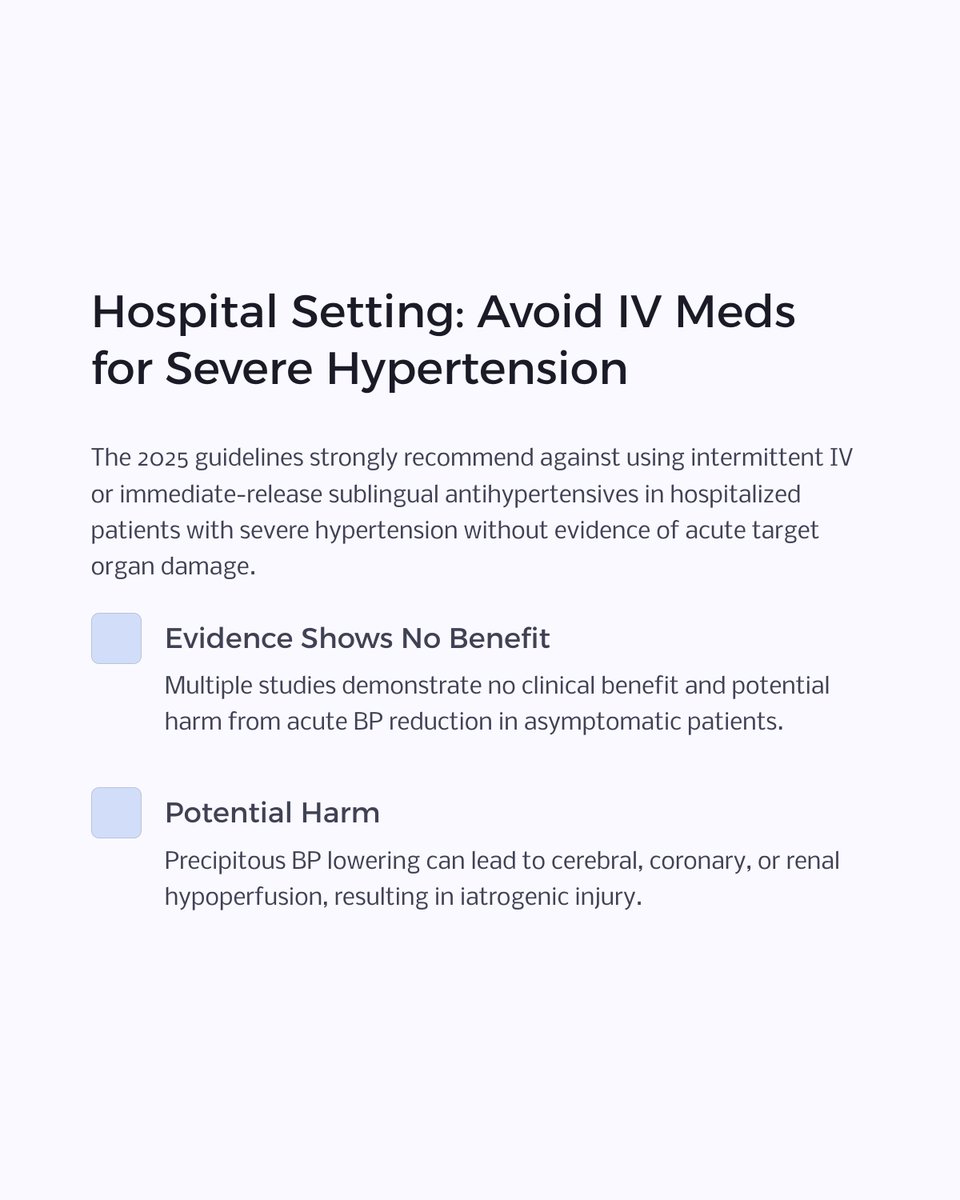
Move away from IV meds for asymptomatic severe HTN. Oral initiation is key.
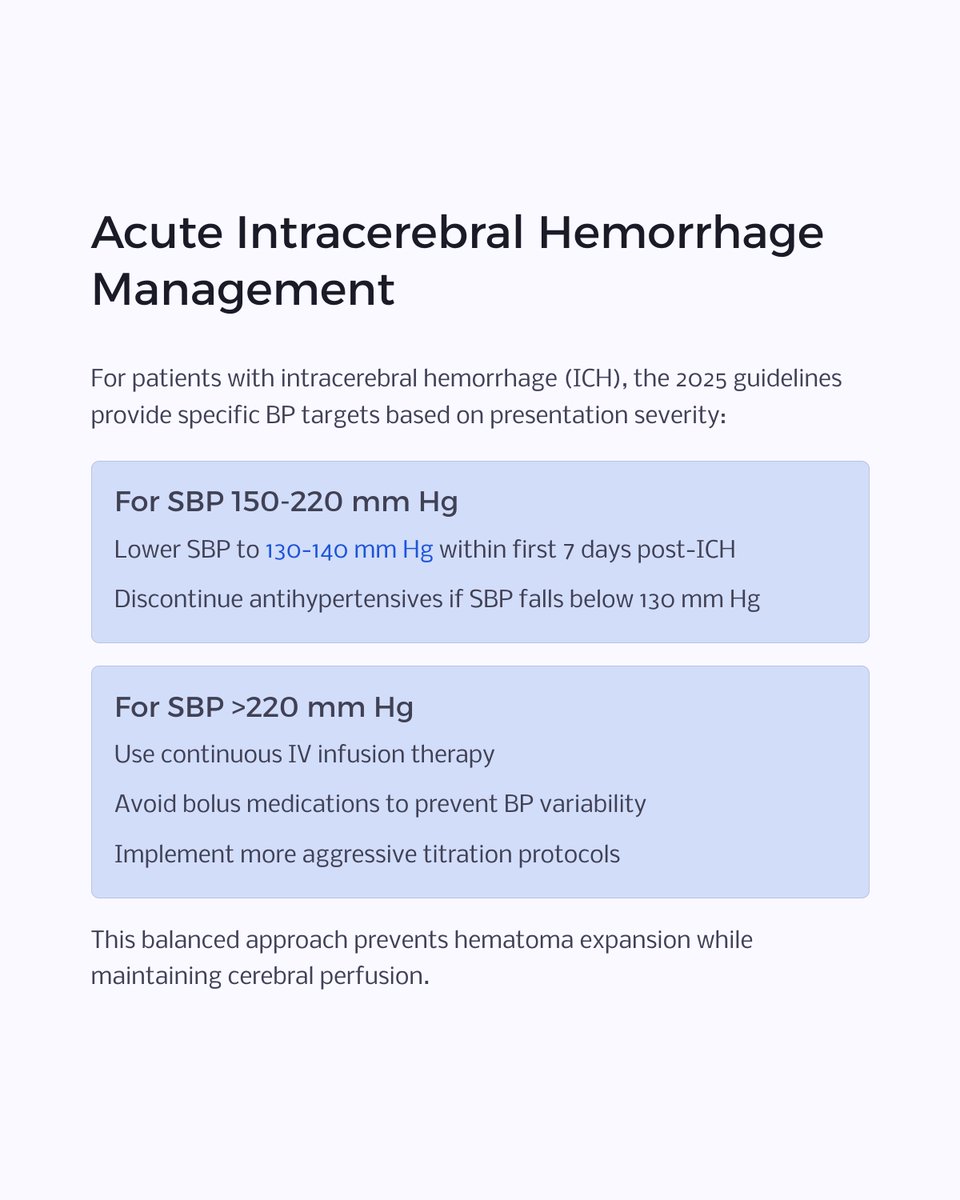
New, specific BP targets for ICH & post-reperfusion ischemic stroke.
The PREVENT risk calculator is in, setting new thresholds (≥7.5% risk) for starting meds at BP ≥130/80.
Swipe through the carousel for a full visual breakdown of these practice-changing updates!

English
SEMily, Char.D. retweetledi

💡 Need one more reason to love your friendly EM pharmacist? Check out this @EMPHARM_NET SR/MA:
⏰ EMP presence was associated with reduced mean DTN time by 14.6 minutes (95 % CI -18.1, −11.1 min)
Time for @American_Stroke @American_Heart to take notice?
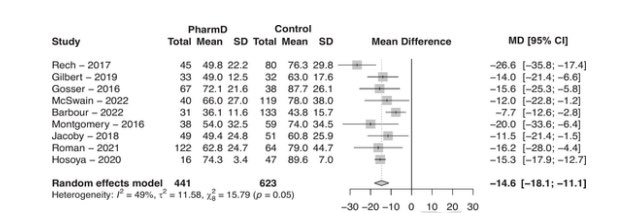
Kevin Mercer, PharmD, MPH@ohsnapimginger
Just published in #AJEM! 📄 #PhAST1 is the first systematic review & meta-analysis quantifying the impact of #EMPharmD on stroke #doortoneedle times 🧠🚑 📉 Faster treatment 🤝 More interprofessionalism 🏥 Justification for expanding #EMPharmD services doi.org/10.1016/j.ajem…
English
SEMily, Char.D. retweetledi

Norepi all day
SCCM Clinical Pharmacy and Pharmacology Section@SCCM_CPP
What is the ideal vasoactive agent after a medical cardiac arrest - Norepinephrine or Epinephrine 💉? Check out this infographic from #SCCMJC to learn more about this study published in Am J Emerg Med! #PharmICU loom.ly/suWhdcQ
English
SEMily, Char.D. retweetledi

It’s time, once again, to enter the realm of TXA (tranexamic acid) in trauma! Recent updates mean we can often give this powerhouse with a quick 1-2 gram IV push, instead of a long, resource-intensive, 8-hour drip. Talk about efficiency!
Plus, at typical trauma doses, you don't need to worry about the "prothrombotic" villain—those studies used a whopping 4g, way more than our heroic doses! So whether you're following the Tactical Combat Casualty Care's 2g guidance or NAESP's 1-2g, remember: TXA is on your side, helping to keep things clotted in all the right places!
#TraumaTalk #TXAFunFacts #emergencymedicine #trauma #EMRAP
English

Which antibiotic is most likely to make a huge bid at an auction?
Macrobid!!!!
English
SEMily, Char.D. retweetledi

Emergency medicine and critical care pharmacists play an integral role in trauma resuscitation/MTP. Our article sums up key information in the management of this patient population. @ASHPOfficial @accpemedprn @SCCM_CPP @EMpharmacists @SAEM_AEMP
pubmed.ncbi.nlm.nih.gov/40580496/
English
SEMily, Char.D. retweetledi
Check out our new segment on anti-amyloid mABs to learn why you need to be aware of these meds in the ED 👇
🧠 ADEs called ARIAs are non-specific, typically require MRI & can mimic stroke
⛔ Concomitant thrombolytics/anticoagulants are contraindicated
annemergmed.com/article/S0196-…
EM:RAP@emrap_tweets
Are you up-to-date on the latest implications of new Alzheimer's therapies for emergency medicine? Anti-amyloid monoclonal antibodies (mAbs) like lecanemab and donanemab are transforming Alzheimer's treatment, but they introduce unique risks. Notably, an increased risk of intracranial bleeding makes them a contraindication for thrombolytics. How does your institution integrate this into your lytics checklist? Sean and Megan discuss best practices for managing patients on these therapies, especially when considering anticoagulation or evaluating neurologic symptoms. #ClinicalPractice #Alzheimers #HealthcareUpdates #EM #EmergencyMedicine
English
SEMily, Char.D. retweetledi
New SRMA in-press with 6 studies comparing re-arrest rates post-ROSC btwn epi and norepi gtts with NE showing lower re-arrest rates and a non-significant increase is survival to discharge
Should likely be doing NE gtts in most everyone post-ROSC at this point

English
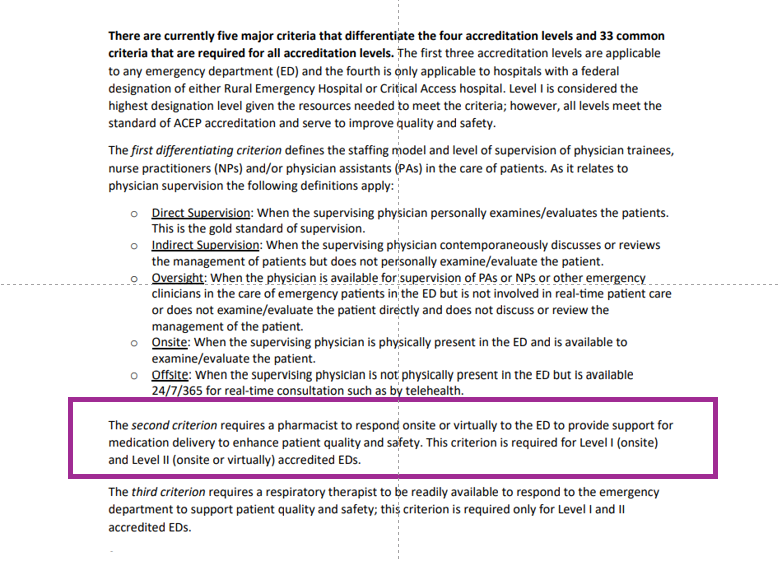
🚨 @ACEPNation ED Accreditation Criteria are out and thanks to @SAEMonline & @SAEM_AEMP a pharmacist is now required for all Level 1 & Level 2 sites - THIS is the work we're doing to advance EM pharmacy practice 👐acep.org/siteassets/sit…
English
@geodonhug @MeganARech @ACEPNation @SAEMonline @SAEM_AEMP @LRayRx @EmergPharm @bfaine1 @KyleWeant @AM_EM_PharmD @EMPoisonPharmD I second this
English
SEMily, Char.D. retweetledi
🔥New @EMPHARM_NET DONT EXPAND Study:
💊Propensity-matched, 11 EDs: desmopressin (n=35) vs. controls (n=140)
😷Desmo patients had higher baseline ICH volumes
🧠No difference in good or excellent hemostatic efficacy assessed via hematoma volume measures
sciencedirect.com/science/articl…

English
@johnson8707 @accpemedprn Best pharmacokinetic profile, fastest control, shortest duration if you overshoot a little bit. Also low fluid burden. We have a lot of CKD and HF where I practice
English

What is your first line antihypertensive used in the setting of ICH?
English