Dr. Shiv_Kumar@Dr_Shiv_kumar_
🚨Cardio-emergency pearls you should never miss as a clinician 7️⃣
In hypertensive crisis, the number misleads. The organs tell the real story lets break this down
🟥 HYPERTENSIVE EMERGENCY
🟨 SEVERE BP (NO ORGAN DAMAGE)
🔻1. Definition (Get this right first)
Hypertensive crisis = BP ≥180/120 mmHg
⚠️ But classification depends on END-ORGAN DAMAGE, not the number:
🟥 Emergency → Acute target-organ injury
🟨 Severe BP → No injury
👉 Same BP. Completely different management.
🔻2. Terminology update
🟨 “Hypertensive urgency” → ❌ obsolete / discouraged
👉 Why?
Misleading → overtreatment → harmful rapid BP lowering
✔️ Use:
→ Severe asymptomatic hypertension
→ Severe BP without organ damage
🔻3. Before labeling a crisis - verify BP. Pseudo-elevation is common.
✔️ Correct cuff size
✔️ Repeat after 5 min rest (seated, back supported)
✔️ Measure both arms (>15 mmHg difference → suspect vascular disease)
✔️ Check for: pain, anxiety, full bladder, recent caffeine/nicotine
👉 Many normalize → avoid unnecessary IV therapy
🔻4. Pathophysiology
Chronic HTN → right-shifted autoregulation
Acute rise → endothelial injury
→ fibrinoid necrosis + capillary leak
→ microangiopathy + ischemia
Rapid BP fall → hypoperfusion → infarction
🔻5. Target Organ Damage (Defines EMERGENCY)
🧠 Neuro → encephalopathy, stroke, seizures
❤️ Cardiac → ACS, LV failure, pulmonary edema
🧂 Renal → AKI, hematuria/proteinuria
👁 Eye → papilledema, flame hemorrhages
🫀 Vascular → aortic dissection
🤰 Obstetric → preeclampsia/eclampsia
🔻6. MAP : what organs actually care about
MAP = DBP + \frac{1}{3}(SBP - DBP)
👉 All targets are based on MAP reduction, not SBP alone.
🟨 SEVERE BP (NO ORGAN DAMAGE)
🔻7. Management (Do less, but do it right)
❌ No IV antihypertensives
❌ No rapid BP reduction
✔️ Start/adjust oral therapy
✔️ Identify triggers (pain, NSAIDs, steroids, non-adherence)
✔️ Reinforce compliance
✔️ Follow-up in 24–72 hrs
⚠️ Rapid lowering here → stroke / syncope risk
🟥 HYPERTENSIVE EMERGENCY
🔻8. Core principle - Controlled reduction:
• 1st hour → ↓ MAP ≤25%
• Next 2–6 hrs → ~160/100–110 mmHg (slight correction)
• 24–48 hrs → gradual normalization
❌ Never normalize immediately
🔻9. Why this matters
Chronic HTN → shifted autoregulation
Rapid drop → hypoperfusion →
→ Stroke
→ MI
→ AKI
🔻10. Condition-specific targets
🫀 Aortic dissection
→ SBP <120 + HR <60 (within minutes)
→ IV beta-blocker FIRST (then vasodilator)
🧠 Ischemic stroke
→ No thrombolysis: allow ≤220/120
→ Thrombolysis:
Before: <185/110
After: <180/105
🧠 ICH
→ Target SBP ≈ 140
→ Avoid <130
💦Pulmonary edema
→ IV nitroglycerin + diuretics
🤰 Preeclampsia/eclampsia
→ Labetalol / Hydralazine
→ MgSO₄ (seizure prophylaxis)
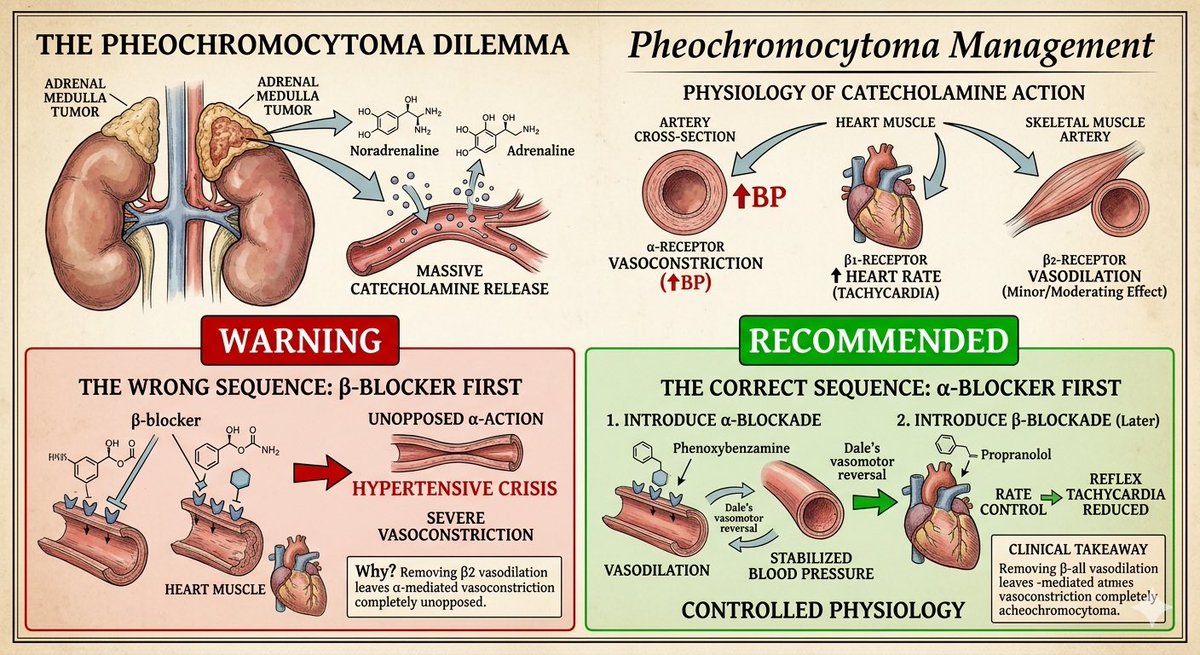
sympathomimetic
→ ❌ Avoid pure β-blockers
→ Use benzodiazepines + vasodilators
🔻11. IV drugs (Know your weapons)
✔️ Nicardipine
✔️ Labetalol
✔️ Esmolol
✔️ Clevidipine
✔️ Nitroglycerin
⚠️ Nitroprusside → last resort (cyanide toxicity & sudden hypotension)
🔻12. Investigations (Don’t miss organ damage)
🧪 Labs:
CBC, creatinine, electrolytes
Troponin, LDH
Urinalysis (protein/hematuria)
Imaging:
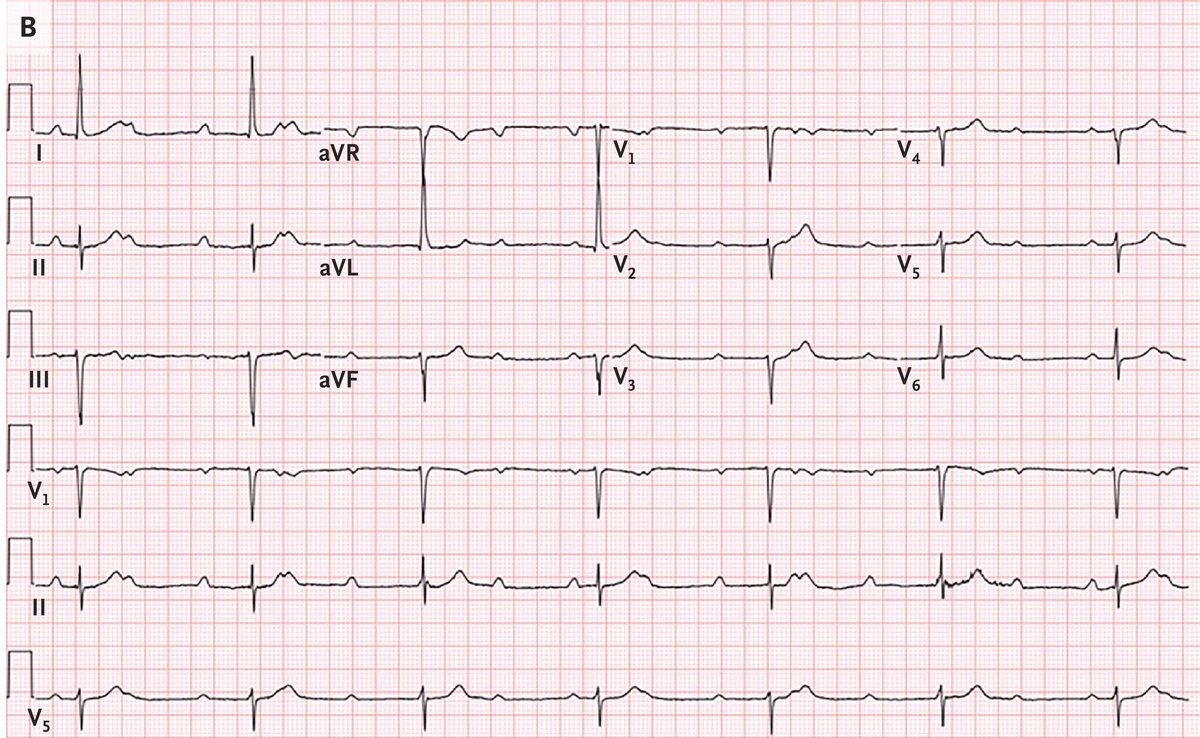
ECG
CXR
CT brain (if neuro signs)
Echo (if cardiac involvement)
🔻BEDSIDE CLINICAL EXAM (MUST DO)
General
Mental status → encephalopathy?
Seizures / confusion
Vitals
BP in BOTH arms
Pulse deficit → Aortic dissection
Eye (Fundoscopy)
Papilledema → emergency
Hemorrhages/exudates
Cardiac
S3 → LV failure
New murmur → dissection (AR)
Respiratory
• Crackles → pulmonary edema
Neuro
• Focal deficits → stroke
Peripheral
• Weak/absent pulses → vascular cause
🔻14. Pitfalls (Exam + real life traps)
❌ Treating numbers blindly
❌ Overcorrection (>25% drop early)
❌ Missing aortic dissection
❌ Giving IV drugs in non-emergency
❌ Not doing fundoscopy
#MedTwitter #MedX #Cardiology