
@BehindTheKnife you guys have a pelvic floor dedicated episode?!?
English
Jada Saunders
124 posts
@JadaS95
Gen Surg SpR North East. Views are my own.





Resident doctors have been left with no choice but to strike. Weeks of negotiations with the Government have failed to deliver enough progress on pay, with the goalposts being moved at the last minute. We have called six days of industrial action to make the Government listen, stop the game playing, and come back with an offer that delivers fairly on both jobs and pay.
You could be in a 2 minute OR i&d and anesthesia will have switched teams 3 times to give eachother a break






"un hospital existe única y exclusivamente para curar enfermos. No sirve para dar empleo ni para justificar organigramas. Tampoco para alimentar burocracias ni para experimentar teorías organizativa" Gran artículo, merece la pena leerlo. farodevigo.es/opinion/2025/1…







@Ryanair leg room to match our gap at the top of the table
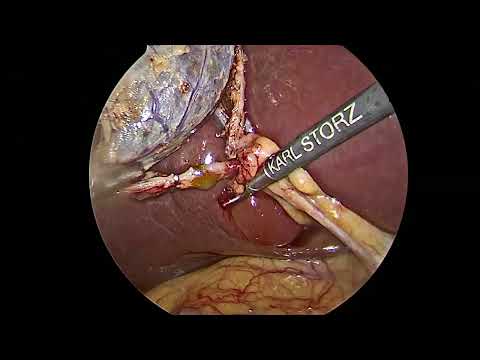
𝗡𝗮𝗿𝗿𝗮𝘁𝗲𝗱 𝗩𝗶𝗱𝗲𝗼: 𝗘𝗺𝗲𝗿𝗴𝗲𝗻𝗰𝘆 𝗟𝗮𝗽𝗮𝗿𝗼𝘀𝗰𝗼𝗽𝗶𝗰 𝗥𝗲𝗽𝗮𝗶𝗿 𝗼𝗳 𝗦𝘁𝗿𝗮𝗻𝗴𝘂𝗹𝗮𝘁𝗲𝗱 𝗢𝗯𝘁𝘂𝗿𝗮𝘁𝗼𝗿 𝗛𝗲𝗿𝗻𝗶𝗮 #FOAMed #GITwitter #MedEd #SurgEd #SoMe4Surgery
What Would You Do 🔴Admission with severe acute pancreatitis 🔴Requirement for ICU support 🔴Acutely unwell and CT performed (Image 1) 🔴Stabilised with organ support and conservative treatment 🔴>4 weeks post index admission ➡️CT and MRCP performed (Image 2 & 3) ➡️Pt now requiring no organ support but ongoing low grade sepsis ➡️Supplementary feeding What is the Dx? What would you do? What would guide your management options?