Sabitlenmiş Tweet

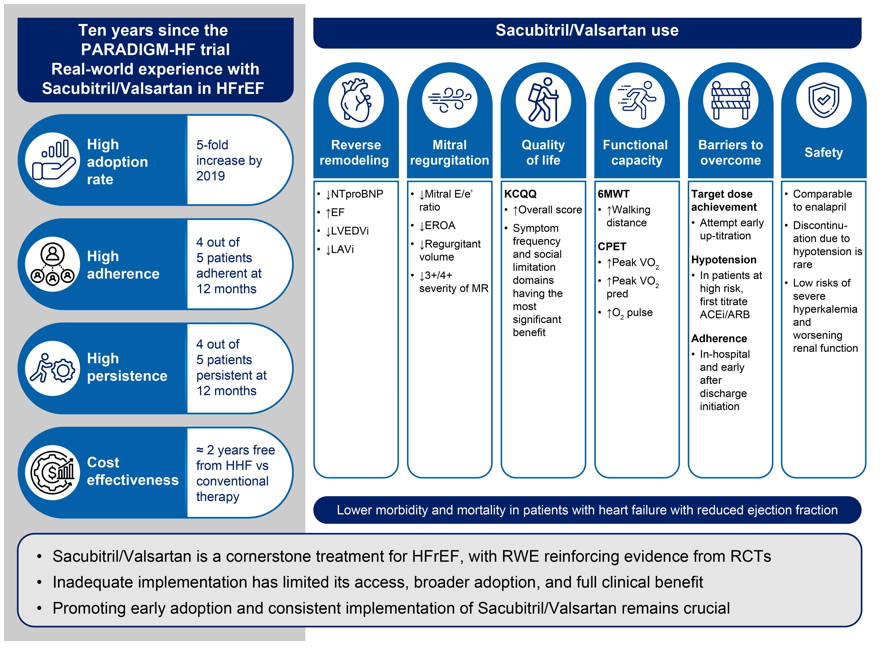
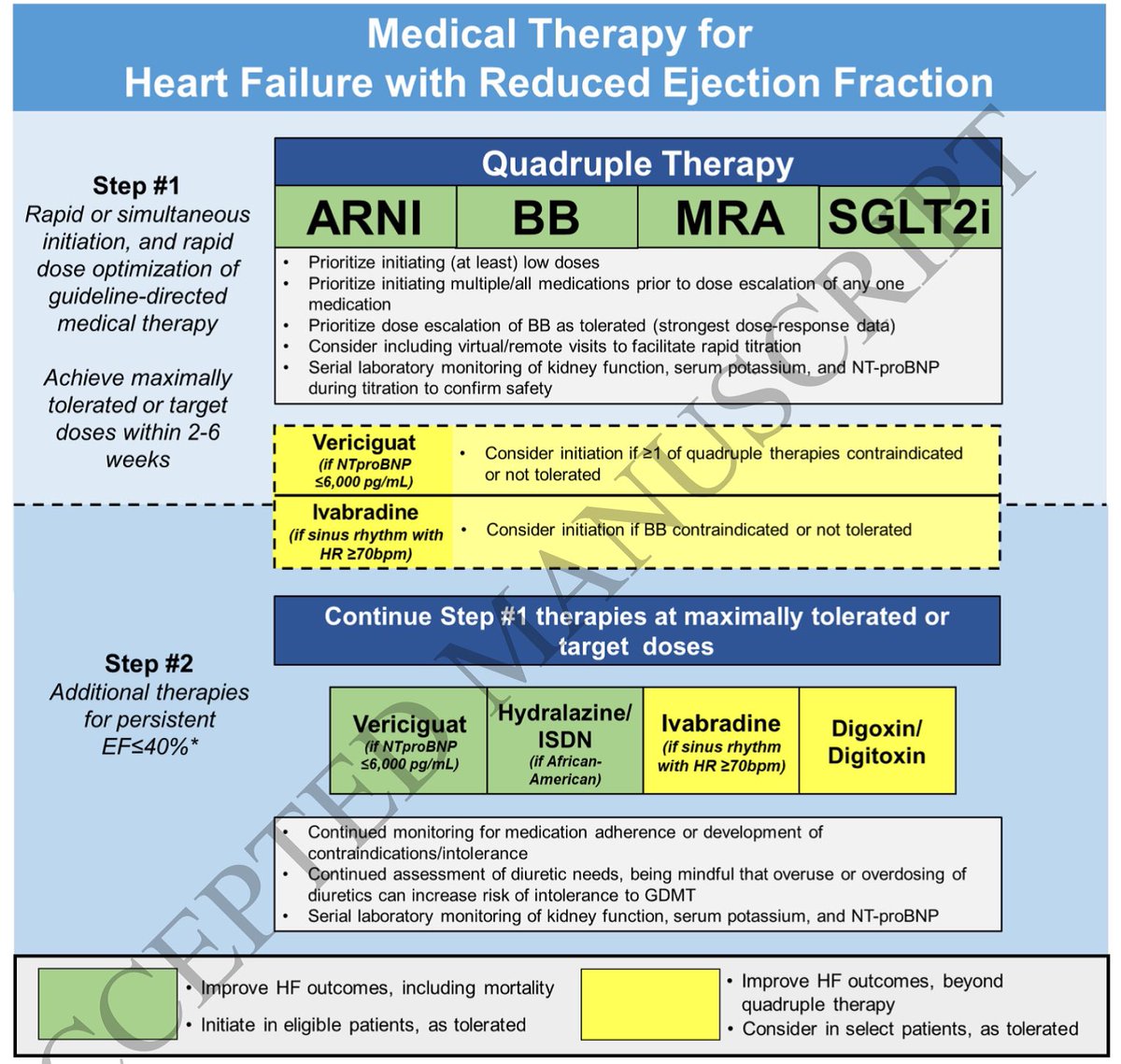
The 3 rules of #GDMTWorks for #HFrEF:
1. Start more
2.⬆️doses
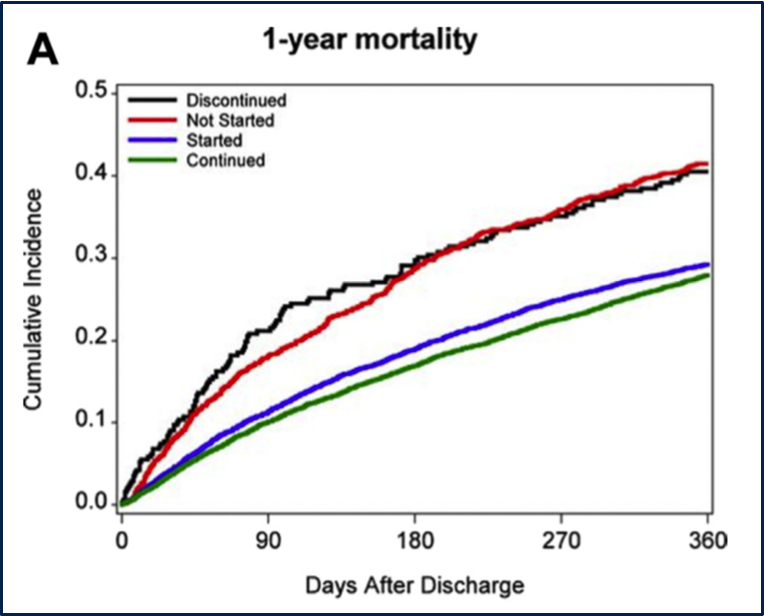
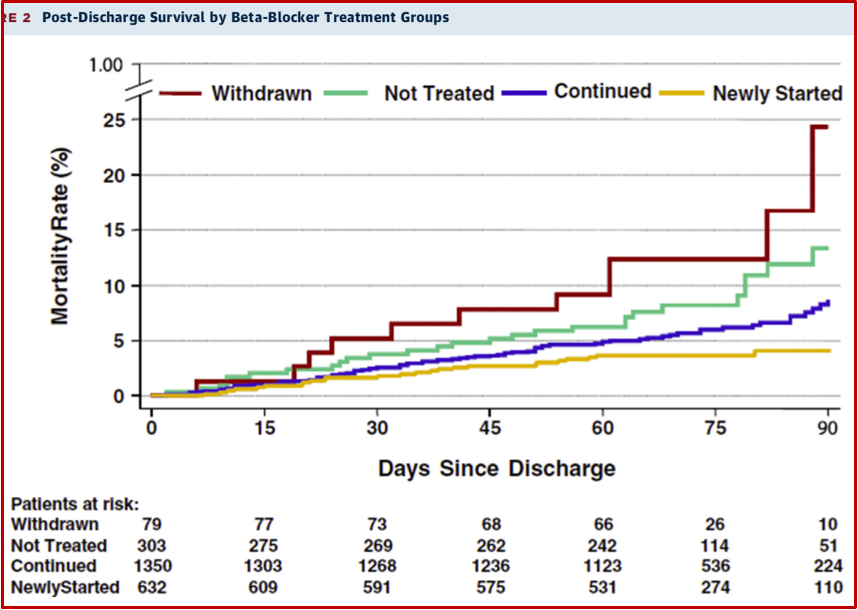
3. Keep them going
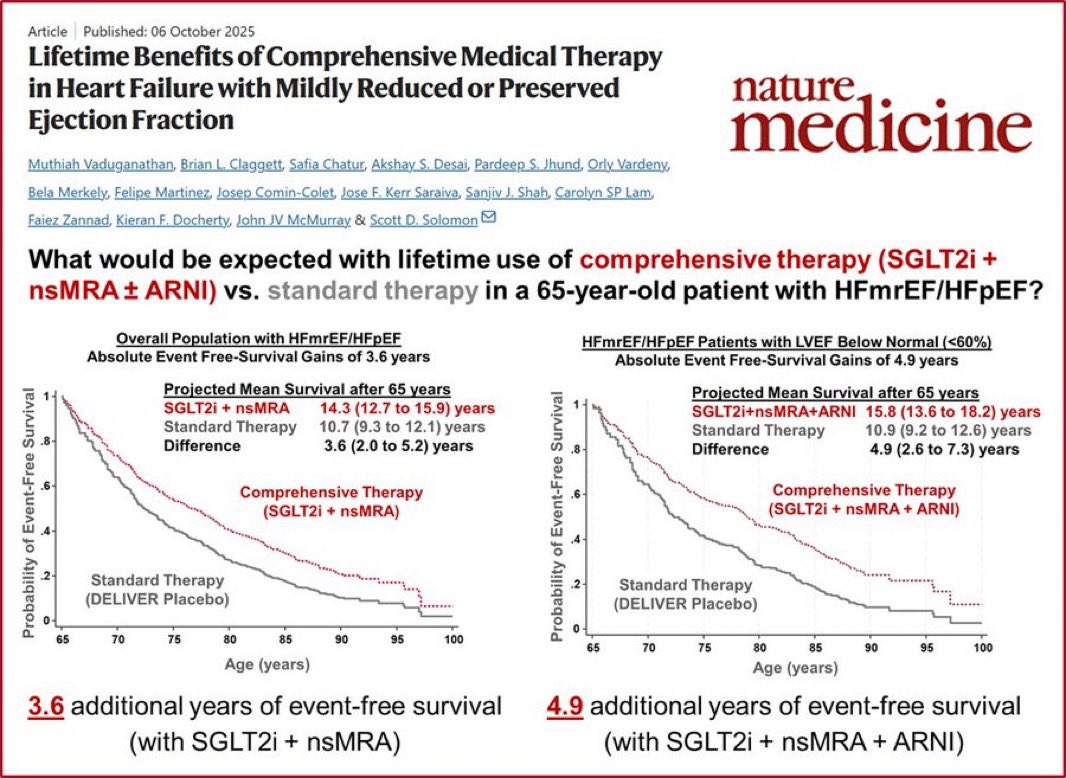
#QuadTherapy: BB + ARNI + MRA + SGLT2-I. 75% RR reduction w NNT of <4!! @gcfmd @MKIttlesonMD @AndrewJSauer @AminYehyaMD @mpsotka @DrNasrien @shwinner @ShelleyZieroth @iamritu @DevinMehta @datsunian
English