Sabitlenmiş Tweet

Why is it vital for humanity to fight aging?
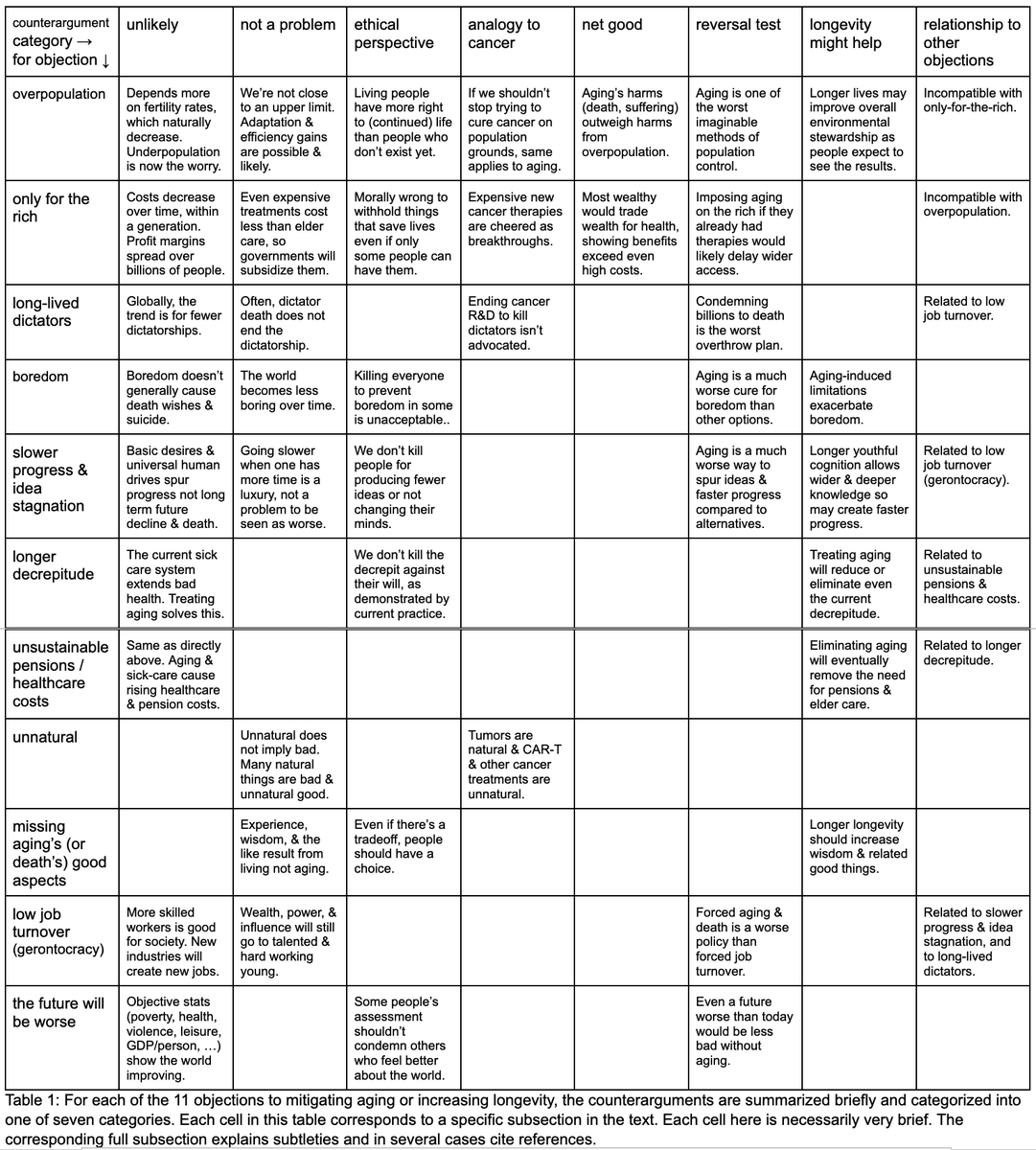
Why are common longevity worries not big problems?
My new review:
zenodo.org/records/188830…
a preprint of a book chapter for the upcoming radical longevity book that many in the field have contributed to.
English













