
Michael Mindrum, MD
23.7K posts

Michael Mindrum, MD
@MichaelMindrum
Internal Medicine & obesity specialist. Born in 🇺🇸, 🇨🇦 is home.
Nova Scotia, Canada Katılım Ocak 2018
2.4K Takip Edilen10.9K Takipçiler

Has anyone else noticed that Eli Lilly's pipeline seems suspiciously focused on making it possible to have a really good weekend in Vegas?
Crémieux@cremieuxrecueil
As a recap on my appearance, Eli Lilly is pursuing: - A one-dose drug for preventing most heart disease - A vaccine for chlamydia - A vaccine for gonorrhea - A vaccine for Epstein-Barr - A drug that lets you stay awake longer and feel more rested It's a golden age of pharma!
English

As I have been saying the future or present of obesity care is combination therapy.
Gastroenterology & Endoscopy News@gastroendonews
Could the future of obesity treatment be combination therapy? 💉🔪 Experts at #ASMBS2025 highlighted how weight-loss medications + bariatric surgery may lead to greater, more durable results: gastroendonews.com/a/dTkBAA/t #GLP1 #obesity
English
@EricTopol @scisignal interesting study... a nightmare of an infographic.
English

By connecting the brain and pancreas, activation of the vagus nerve increases insulin release after eating. But with obesity the opposite occurs!
Now we know why (NO-nitric oxide, Nos-nitric oxide synthase, KO-knockout). From experimental model work @scisignal
science.org/doi/10.1126/sc…

English
Interesting study and absolutely horrible infographic.
Eric Topol@EricTopol
By connecting the brain and pancreas, activation of the vagus nerve increases insulin release after eating. But with obesity the opposite occurs! Now we know why (NO-nitric oxide, Nos-nitric oxide synthase, KO-knockout). From experimental model work @scisignal science.org/doi/10.1126/sc…
English
Michael Mindrum, MD retweetledi

1/5
I'm a cardiologist. I have spent twenty years watching cholesterol destroy arteries, trigger heart attacks, and kill people I care about.
Today, Eli Lilly presented data that may begin to end that era.
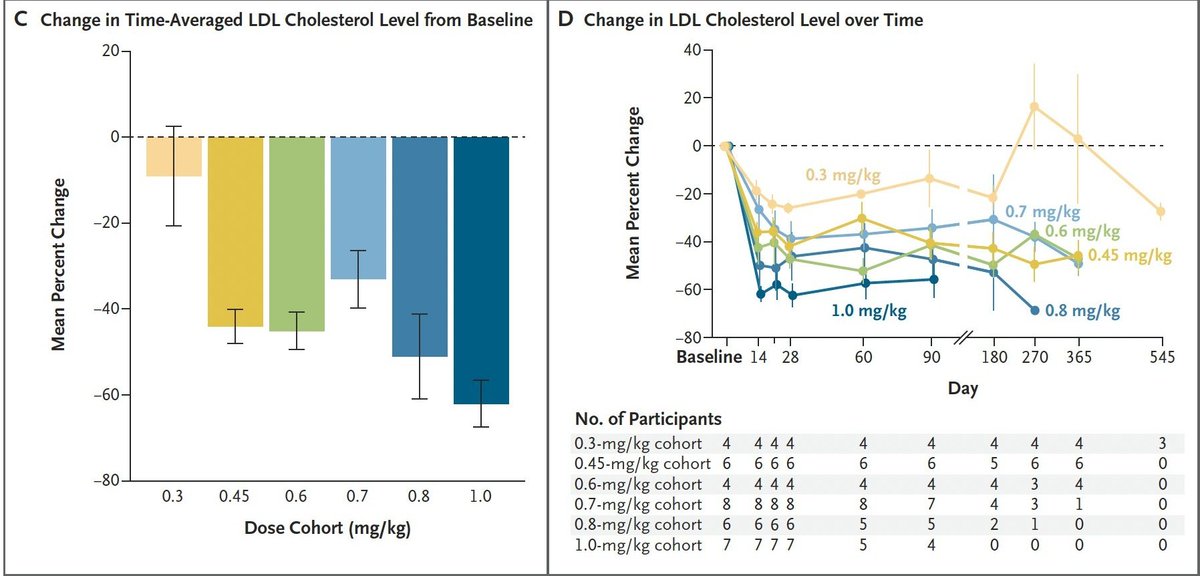
VERVE-102. A single infusion. One dose. It uses base editing to permanently turn off the PCSK9 gene in your liver.
Presented today at the European Atherosclerosis Society Congress:
88% reduction in PCSK9.
62% reduction in LDL cholesterol.
Sustained up to 18 months.
No treatment-related serious adverse events.
One infusion. Not daily pills you forget to take. Not monthly injections. One dose — and your cholesterol may stay low for the rest of your life.
English
@MartinShkreli @0xMasonH Why do you say not that valuable?
English

@0xMasonH eh this is not that valuable, no one wanted it, lilly didnt pay much for it
English

It's a shame that this is likely 6-8 years from hitting the market
Crémieux@cremieuxrecueil
Eli Lilly has done it. They've gone and made what seems to be a powerful, permanent gene therapy for LDL cholesterol. That means they'll be able to effectively prevent most heart disease with a single infusion!
English
Color me surprised!
Eric Topol@EricTopol
For people with poorly controlled Type 2 diabetes ("early," within 4 years of diagnosis), a randomized trial of tirzepatide vs intensified conventional care (ICC). Tirzepatide was superior for achieving glycemic control and all secondary endpoints @AnnalsofIM acpjournals.org/doi/full/10.73…
English
The curse of delusions and mass hysteria strikes again.
MD@mike_daddino
I promise… this is the most astonishing video you will see today
English
Michael Mindrum, MD retweetledi


@MichaelMindrum When you come by GLP1s with several of the older medications you end up with incredible amounts of weight loss beating bariatric surgery and keeping the weight off forever.
English
We still have a long way to go to treat and manage obesity effectively. We need more access to surgery and to medical therapy.
Medical therapy has downsides: many people don't have access, and many others discontinue treatment within a year. There are side effects to contend with, a lack of proper medical supervision for many, a lack of education and unreasonable expectations, cost, lapses in insurance, and intentional barriers set up by insurers.
Even when the response is excellent, a significant portion of patients would benefit from further reduction in adiposity to improve their obesity-associated complications. These patients would benefit greatly from bariatric surgery, with or without drug therapy.
Writing a prescription is easy. Creating a pop up telehealth pill-mill company selling drug to vulnerable population without proper medical supervision is profitable.
Discussing obesity as a complex chronic disease, sharing with a patient the brain biology of obesity, explaining how different interventions fit into long-term weight management, setting reasonable expectations, and matching the intervention to the disease takes expertise, time, and patience. For some behaviour change is perfect, others will benefit from drug therpy, others bariatric surgery, and others will benefit from all of the above. It needs to be a rational and well - understood process.
The medical system needs to be arranged in a way that reduces the friction between a patient's disease state and effective treatment pathways: longitudinal programs informed by behaviour change psychology, proper medication supervision, cohesive and seamless referral pathways to bariatric surgery, and access to surgeons who have adequate time and support to perform surgeries at increased scale.
We still have a long way to go.
Neil Floch MD@NeilFlochMD
GLP1 substantially reduce the popularity of #bariatricsurgery at least for now but surgery will continue to have a role when less than 50% of patients respond with similar results
English
Michael Mindrum, MD retweetledi

It feels very futuristic to imagine a world with one-and-done therapies that lower LDL cholesterol for life, but... it might not be far off!
These are new phase 1 data for Verve/Lilly's PCSK9 base editor: one single intravenous infusion reduces LDL cholesterol by as much as 60%

English
Michael Mindrum, MD retweetledi
Michael Mindrum, MD retweetledi

The difference between people in long lived populations and those with chronic disease in western populations is not willpower. It’s the environment. If you take those same people from long live populations and expose them to the western environment many of them become obese.
Does everyone have the same genetic vulnerability? No. Which is why some people can remain thin despite the environment.
Scott@Mustang_Scott
@cremieuxrecueil wtf are you talking about We need willpower and a decent food supply The willpower applied to exercise and eating properly also applies to going out and working and being productive
English
@terrysimpson So glad we have many more tools that we had just 15 yrs ago but it can be a stubborn, frustrating, and at times devastating dz. I think we need to treat early and aggressively
English

@MichaelMindrum It is great when any can reverse disease for a bit - we saw this in patients with weight loss surgery -about 75% whose diabetes was found in the 2 years previous. Sadly with time some DM came back. Horrific disease
English
Some of my “Star” patients who placed their diabetes in remission with keto 5 to 8 yrs ago are coming back to see me due to diabetes rearing its ugly head again. These are among the most motivated of the motivated. The stubborn shadow of type 2 diabetes follows and it needs to be respected and not judged.
Dr Terry Simpson@drterrysimpson
This is not true. Diabetes is a disease that can be made worse with a bad diet, but cannot be "cured." You cannot regrow islet cells that produce insulin. Some can go into remission, but cannot be "reversed."
English
Anybody else notice that one Claude interface has very littel understanding what other Claude interfaces can do (i.e. Code, Co-work, and Web). It can be a bit confusing.
English

@alt_w_v_g Could you analyze the ROI of marital counseling in your situation?
English

My wife mentioned a nice private school over dinner this week
She said the campus was beautiful
I asked what's the tuition
She said we should look at it as an investment in him not a cost
I made a note
She said don't make a note
I said I always make notes
She said this isn't a deal
I said everything is a deal
She closed her eyes
She said we'd discuss it Saturday
I agreed
Saturday 7:02am
She came downstairs in her Saturday robe
Coffee in hand
I had my cargo shorts on
The dining room had been cleared
The projector was on
The analyst was at the head of the table
Quarter zip on, three iced coffees, a legal pad, and two laptops
He had been there since 6:44am
I texted him at 11:14pm Friday
The text said dining room 6:45am bring the model
He sent a thumbs up
My wife stopped in the doorway
She said what is this
I said you said you wanted to discuss it
She said this is not a discussion
I did not respond
She sat down anyway
The analyst stood
He said good morning ma'am
She did not respond
He sat back down
A printed deck in front of each seat
A fourth copy in case
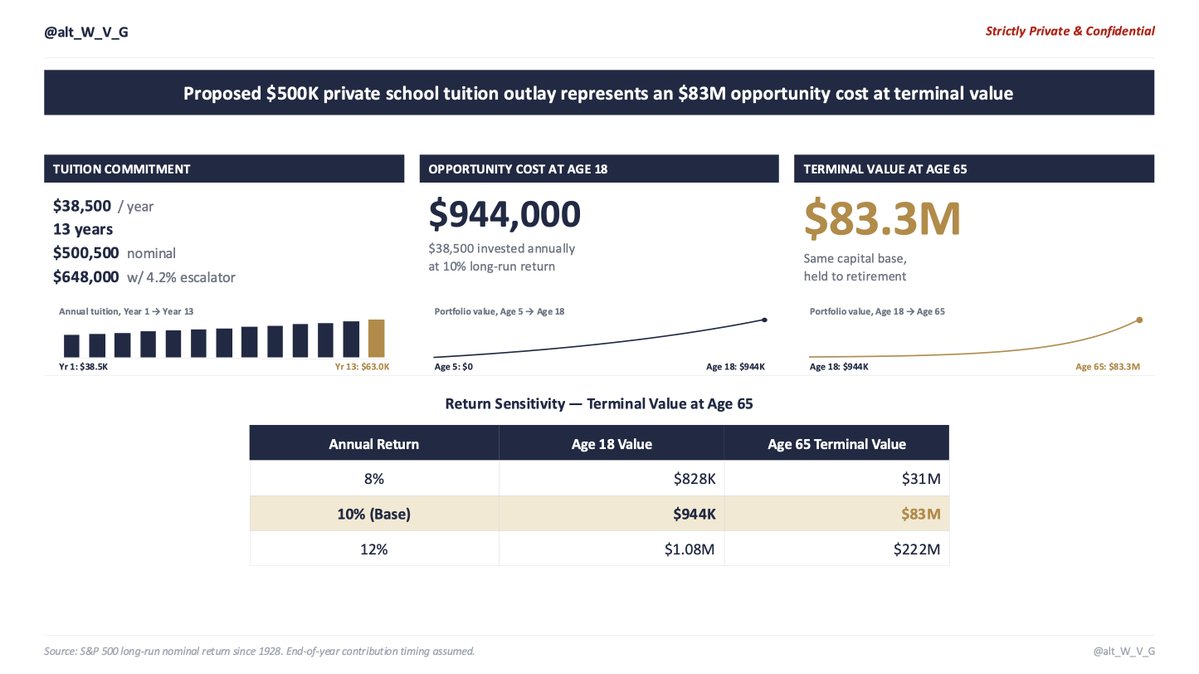
Slide 1 Tuition Schedule
$38,500 per year
Thirteen years
$500,500 nominal
Before escalators
The school has raised tuition 4.2% per year for a decade
With escalators $648,000
My wife said okay
I said I'm not done
Slide 2 Opportunity Cost
Even before escalators
$38,500 invested annually
10% nominal return
S&P long-run average since 1928
By his eighteenth birthday $944,000
My wife said we can afford it
I said I know that's not the slide
Slide 3 Terminal Value at Age 65
$83 million
She was quiet
The analyst slid the sensitivity tables across the table
8% return $31 million
10% return $83 million
12% return $222 million
She did not look
She said this isn't about money
I said it's always about money
She said no it isn't
I said then what is it about
She did not answer
She said you can't put a dollar value on his teachers his classmates his environment
I said I can the analyst already did slide 6
He flipped to slide 6
She did not look
She said the school is the best in the city
I said best is a feeling
She said it produces the best students
I said the students were already the best before they got there
She said our son deserves it
I said our son deserves $83 million
My son walked in
He is five
Dinosaur pajamas
He looked at the projector
He looked at the open deck on the table
He looked at slide 3
He said are we modeling pre-tax or after-tax
The analyst opened a new tab
My wife looked at the ceiling
He said what's the discount rate
The analyst set down his pen
She closed her eyes
He said is this the same return assumption from the 529 conversation
The analyst stopped typing
He looked at me
I did not say anything
She stood up
Sat back down
He said dad can I help
I said yes
He pulled up a chair
The analyst handed him a printout
He started reading
My wife watched him read
She watched him for a long time
She said his name
He looked up
She said do you like school
He said the work is too easy and the kids don't ask questions
She did not respond
She looked at the ceiling
She walked out of the room
The analyst started packing up
He said should I follow up Monday sir
I said no follow up needed
He'll be fine
Sent from my iPhone
English
Michael Mindrum, MD retweetledi

Ozempic is about to go generic for billions of people, including in India and China.
The weight loss #obesity drug sold as Ozempic and Wegovy will soon go generic in countries that are home to 40% of the world’s population, significantly lowering the #price of a costly medicine.
nytimes.com/2026/03/19/hea…
English
Michael Mindrum, MD retweetledi

1/ Some things I've learned recently running coding agents on large-scale projects. Most of this contradicts advice from 6 months ago!
English