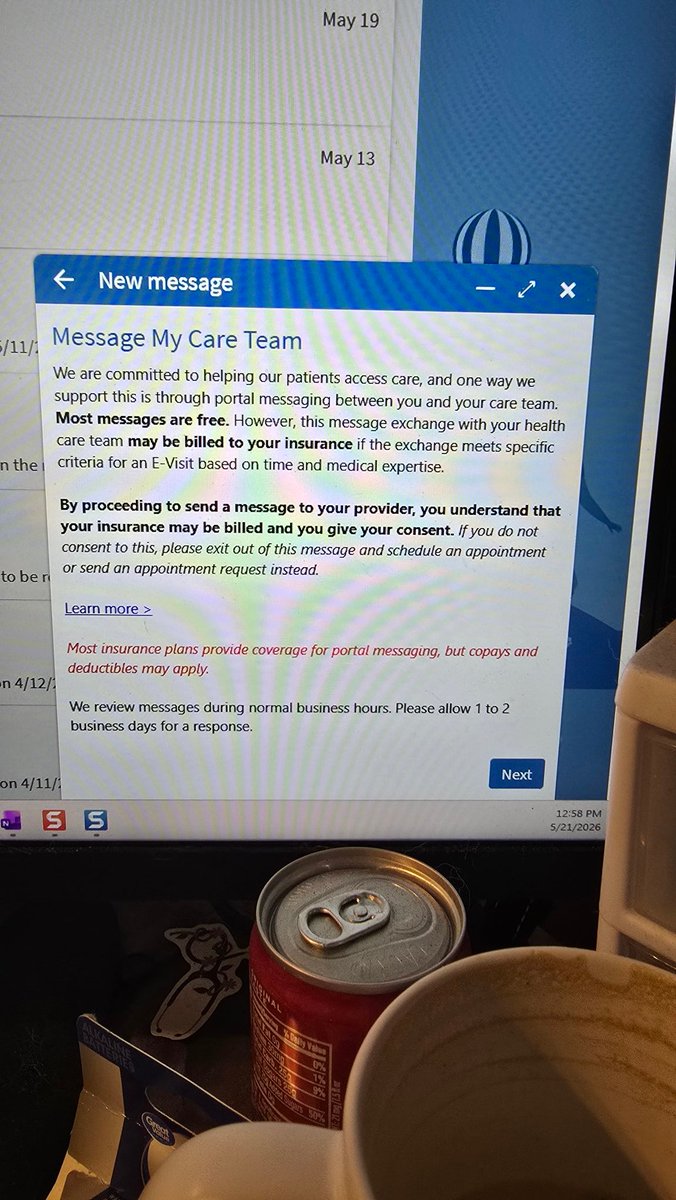
@twomewtoo @DrDiGiorgio @Chillcatser @MaryBowdenMD This is another example of how patients are misinformed and wrongly accuse doctors of greed due to employer actions. The doctor does not get the money paid for MyChart messages-the employer does.
English