Sabitlenmiş Tweet
MedUniDoc
150 posts

MedUniDoc
@MedUniDoc
🩺 Medical Research & Clinical Science (Lvl. 5) 🧬 Focus: Chronic Inflammation & Mitochondrial Health 🔬 Translating complex PubMed data into daily protocols.
Decentralized Medicine Katılım Ağustos 2025
54 Takip Edilen53 Takipçiler
daily use is actually the key variable the single-session studies miss.
the immune benefit compounds IgA, IgG, IgM baseline elevations only appear after serial exposure, not one-offs.
and "life and spark to my years" is the most honest framing of the longevity goal i've seen in a while.
English

@MedUniDoc @foundmyfitness Good to know. I go everyday in my infrared sauna at 175 F, for 30 minutes.
Perhaps there is more hope for me yet 😉🤗
Best investment I made for my health not longevity . Although I'll gladly add some life and spark to my years
English

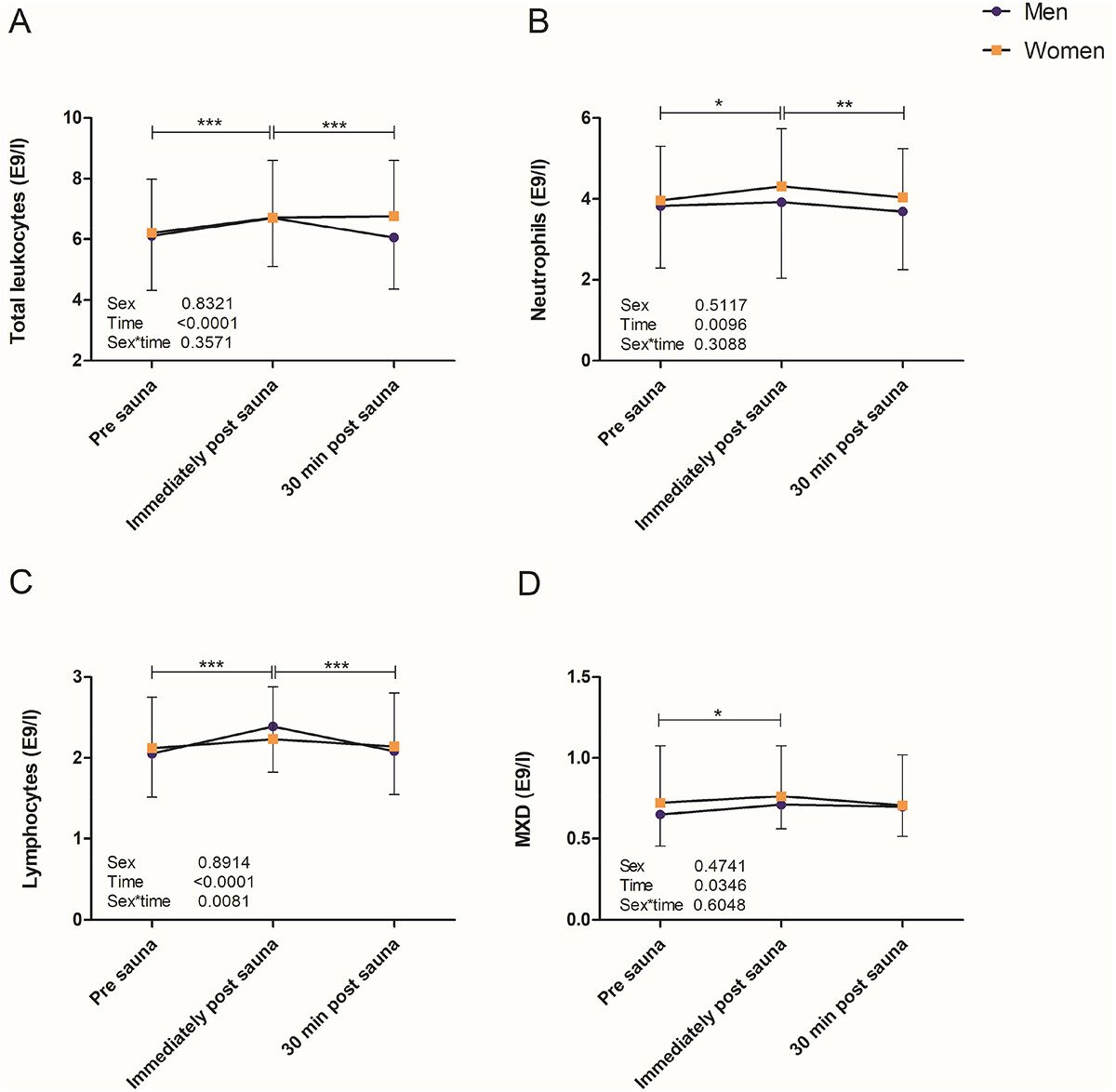
Sauna bathing mobilizes circulating immune cells.
A single 30-minute session at ~165°F (enough to elevate body temperature to 101°F) increased levels of several immune cells including lymphocytes and neutrophils for up to 30 minutes.
This occurred in non-users and people who used sauna 2-3 times per week more.
They also found that changes in more than a dozen cytokines were correlated with body temperature changes, suggesting that the heat stress matters for determining the magnitude of the immune response to sauna.

English
@FirstDoctor @KhandaniM and the ones who do are still being told it's a willpower problem.the gap between what the literature says and what people are told is getting embarrassing.
English

@MedUniDoc @KhandaniM Most people still have no idea what's going on.
English
BREAKING: Half of US adults will be obese by 2030. Not 2040. In 4 years.
English
the absolute vs relative distinction is doing a lot of work here.
yes, absolute muscle mass drops slightly. but as a fraction of total body weight, lean mass goes up because fat loss dominates.
the March 2026 Cell Reports Medicine data showed something else too: GLP-1 treatment increased mitochondrial proteins in muscle compared to calorie restriction alone. the muscle isn't just preserved it's metabolically remodeled.
the caveat nobody adds to these discussions: without resistance training and adequate protein, the picture changes fast.
English

Excellent discussion on effect of GLP-1 based weight loss on skeletal muscle.
Lean mass and skeletal muscle with GLP-1 medicines relative to total body weight increased. Functional tests largely improved.
Learnings from preclinical and clinical data.

MetaboliccareToday.com@MetabolicCare
Do GLP‑1 weight loss drugs harm muscle? Discussing their recent study, Keith Baar (@MuscleScience) and @HenningLanger explain why the concern emerged and what new human and animal data actually show. docwirenews.com/post/glp%e2%80… @UCDavisHealth @ChariteBerlin @CellRepMed @MWeintraubMD
English
nobody talks about the FSH number and it's the most interesting part of this data.
tight underwear raises scrotal temperature, testes detect the damage, and the pituitary responds by pushing FSH higher to compensate. when the researchers adjusted for FSH levels the sperm differences basically disappeared, meaning FSH was the mechanism connecting underwear choice to sperm quality the whole time.
your underwear is having a conversation with your brain you didn't know was happening.
English

Spot on, and "blunted" is doing a lot of heavy lifting.
in many cases the signal is still being sent. leptin levels are elevated. GLP-1 gets released.
but the receptor stopped listening years ago.
it's resistance, not absence. and that distinction matters for how you approach fixing it.
English

@MedUniDoc @FirstDoctor yep. calories still matter, but they stop being the useful lens once the satiety signaling is wrecked. if glp-1 and leptin tone are chronically blunted, telling people to just use willpower is basically asking cognition to override broken sensing
English
the split-dosing insight is the practical takeaway, but there's a second demand-side scenario most people miss.
the adrenal glands hold the highest tissue concentration of vitamin C in the body. during acute stress, ACTH triggers rapid ascorbate release before corticosteroid secretion even begins, vitamin C is a cofactor in the 11β-hydroxylase reaction that converts 11-deoxycortisol to cortisol.
for athletes and anyone under chronic HPA load: the demand curve shifts long before you're sick. 200mg/day doesn't cover that.
English

Most people who take vitamin C take 1,000mg in a single pill. Most people who criticize that dose say absorption drops above 200mg so you're wasting your money. Both groups are missing the more interesting part of the data.
Levine et al. (1996, PNAS) conducted one of the most rigorous vitamin C pharmacokinetic studies ever done. Seven healthy men were hospitalized for 4 to 6 months on a diet containing less than 5mg of vitamin C per day. They were then repleted at seven sequential doses from 30 to 2,500mg, with steady-state plasma concentrations measured at each level.
The absorption curve is sigmoidal. Bioavailability is complete (100%) for a single 200mg dose. At 500mg it drops to roughly 73%. At 1,000mg it drops to roughly 50%. At 1,250mg it is approximately 33%. The intestinal transporter SVCT1 saturates, renal excretion increases, and the fraction you absorb declines with every step above 200mg. Levine et al. (2001, PNAS) confirmed the same pattern in 15 women.
This is the part most people stop at. It's also where the analysis gets lazy.
The fraction drops, but the total milligrams absorbed still increases. At 200mg you absorb about 200mg. At 500mg you absorb about 365mg. At 1,000mg you absorb about 500mg. You are absorbing more vitamin C at every dose increase. You are just doing it less efficiently per milligram. Less efficient is not the same as useless.
This matters because of what happens on the demand side. Immune cells, particularly neutrophils, monocytes, and lymphocytes, actively concentrate vitamin C to levels 50 to 100 times higher than plasma through SVCT2 transporters. In healthy people consuming at least 100mg per day, intracellular concentrations reach roughly 1.5 mM in neutrophils and 3.5 mM in lymphocytes. These cells saturate at about 100mg daily intake under normal conditions.
But conditions are not always normal. During infection, inflammation, surgery, or critical illness, plasma vitamin C can drop below 30 micromol/L within days. Activated neutrophils burn through vitamin C during the oxidative burst, taking up oxidized dehydroascorbic acid via glucose transporters and reaching intracellular concentrations as high as 10 mM. The body pool, roughly 1.5 to 2 grams total, can be substantially depleted during severe illness. At that point, the rate of consumption exceeds what a 200mg dose can replace.
This is the argument for higher doses during illness. Not that absorption is efficient. It is not. But that the absolute amount reaching your bloodstream is still higher at 500 or 1,000mg than at 200, and during periods of high demand, that additional supply maintains the plasma floor your immune cells draw from. The Cochrane review on vitamin C and the common cold (Hemila & Chalker, 2013) found that regular supplementation (200mg to 2g daily) reduced cold duration by 8% in adults and 14% in children, with larger effects in those under physical stress.
The practical insight is not about whether to take more. It is about how to take it.
200mg taken five times per day delivers approximately 1,000mg absorbed, because each individual dose falls within the range of complete bioavailability. 1,000mg taken once per day delivers approximately 500mg absorbed, because the single large dose exceeds SVCT1 saturation.
Same total dose. Roughly double the absorption. If you are going to take a gram of vitamin C per day, splitting it into smaller doses across the day is a straightforward way to get more of it into your body.
For most healthy people eating a reasonable diet, 200 to 400mg per day is sufficient to saturate plasma and immune cells. Supplementation beyond that has diminishing returns under normal conditions. But during acute illness or high physical stress, the math changes because the demand side changes, and split dosing becomes the most efficient way to meet it.
Levine et al., PNAS, 1996
Levine et al., PNAS, 2001
Hemila & Chalker, Cochrane Database Syst Rev, 2013

English
the mechanism goes deeper than most people realize.
HBOT at 2 ATA triggers mitochondrial biogenesis, upregulates VEGF/ERK signaling for angiogenesis, and reduces TNF-α mediated neuroinflammation.
it's not just "more oxygen." it's a pressure-oxygen combo that activates repair pathways cells can't reach under normal conditions.
English

Oxygen is the forgotten nutrient. You can go weeks without food, days without water, but only minutes without oxygen.
HBOT supercharges your cells with oxygen, fueling faster healing, better cognition, and longevity.
English
Greg nails it.
the mechanism most miss: GLP-1 receptor neurons in the hypothalamus are supposed to fire after eating and send one signal "done, stop looking for food."
in a lot of people that signal is broken. not weak. broken.
so the brain keeps searching. not because of hunger. because the off-switch never flipped.
GLP-1 drugs don't blunt appetite. they fix a signal that was never working properly.
English

The Most Powerful Mechanism for Fat Loss Is Not What You Think
Calories in versus calories out. Yes. Law of thermodynamics. We know this.
So why do some people find fat loss a constant battle while others just get lean almost by accident?
The fitness industry says it’s laziness versus effort. That’s bullshit. You know the person who struggles to eat enough and stays lean without trying.
You know the person grinding in the gym, running in circles, getting nowhere. Trying desperately to control calories but going over no matter how hard they try.
The real answer is satiety signaling.
When satiety signaling is downregulated, there is a constant background search for food that never shuts off.
Getting lean feels like swimming against a strengthening current. You restrict, hunger fights back harder, and eventually the pull wins.
When satiety signaling is dialed in, you eat, fullness arrives, food completely leaves your mind, and fat loss just falls into the background of your life. You get lean and you barely notice it happening.
Two completely different biological experiences. If you are in the first bucket and fat loss feels natural and automatic, you do not need any additional support.
But if food is a dominant force in your life, if the noise never shuts off, if every cut feels like a war you keep losing, then not using a low dose GLP tool at this point is a mistake
English
@hubermanlab @ncrawfordmd most women find out their AMH is low when they're already trying to conceive and things aren't working.
but that number can tell you years in advance. before the urgency. before the stress.
early information is the most underused fertility tool there is.
English
the choice exists, agreed.
but try making that choice when ghrelin has already shut off your GLP-1 brake signal and your brain is running a hunger program it literally cannot override with willpower.
same biology that makes GLP-1 drugs work so well. they don't fix laziness. they fix a broken off-switch
English

These are not the same.
You can say it would make them miserable. You can say it would distract them from other things. You can say their body and mind won’t function well if they do it.
But “be in a deficit” is in fact a thing you can choose in a way “have more energy” is not.
MedUniDoc@MedUniDoc
@BioLayne telling someone with impaired GLP-1 secretion and elevated ghrelin to 'just be in a deficit' is like telling someone with hypothyroidism to 'just have more energy'. the physics are correct. the biology is missing.
English
Layne's point is that they weren't actually in a deficit. agreed.
my point: why they couldn't achieve one matters.
GLP-1 doesn't just "force a deficit." it repairs broken satiety architecture, GLP-1R signaling in the hypothalamus, VTA, nucleus accumbens. reward circuitry included.
for some people willpower was never the variable. biology was.
English

English

Them: "I ate in a calorie deficit but didn't lose weight!"
Also them: "I took a GLP-1 and finally lost the weight!"
Who is going to tell them?
Should I tell them????
English
huge appetite since birth isn't a personality trait that's hunger signaling running loud from day one. could be ghrelin, could be leptin sensitivity, could be reward circuitry. the biology varies.
what you did is train the brain to override it consistently until the new pattern became the default.
and honestly? vanity is a completely underrated motivator. the brain doesn't care why it cooperates, just that it does.
English

@MedUniDoc @BioLayne A lot of it is habit. I have had a huge appetite since birth. I can eat 5,000 calories in one sitting. I’m also vain and love clothes. I trained myself to eat moderately and it’s no longer difficult.
English
the honest answer is that after 55 years, a standard TSH won't tell you much.
what actually matters is fT3 the active hormone your cells use and whether rT3 is competing with it. you can have a "normal" TSH and still have tissues running on empty.
when you see a doctor next, ask specifically for fT3, rT3, and reverse T3 alongside the standard panel. not every doctor will order it but the ones who understand thyroid physiology will.
that's the conversation worth having.
English

@MedUniDoc @sith_holocron @BioLayne I know you can't give specific medical advice but anything would help. Thanks just for the conversation. I've never had this kind of convo with someone who actually knows what they are talking about
English
the drop isn't just aging.
visceral fat drives aromatase activity testosterone gets converted to estrogen before it can do anything useful. chronic inflammation suppresses LH signaling at the top of the axis.
the reference ranges are falling because the average male is getting more inflamed, not older.
English
Mean testosterone levels by age group in the US. This is pretty brutal tbh
∙20–24: 409–558 ng/dL
∙25–29: 413–575 ng/dL
∙30–34: 359–498 ng/dL
∙35–39: 352–478 ng/dL
∙40–44: 350–473 ng/dL
Indonesia

how do I lift heavier, be in a calorie deficit, take mg, o3, 100gm protein, regulate cortisol, do skincare, walk 10k steps, do pilates, balance hormones, do sauna, sleep for 8 hrs, regulate emotions, not fall sick WHILE excelling at career & social life & travels & love???
English
yes, that's exactly what I'm saying and the mechanism is documented.
metabolic adaptation: lose weight → leptin drops → NEAT decreases, BMR drops, sometimes T3 drops. the body quietly closes the deficit gap without you changing anything.
the food scale stays accurate, the expenditure side moves. that's why the deficit that worked at week 1 doesn't work at week 12.
English

@MedUniDoc @swellagantP @BioLayne I’m not clear on what you’re saying. Are you saying these are consuming less calories than they are expending and still not losing weight? If not, I’m not sure how this contradicts anything. Yes, based on typical assumptions you may think you are in a deficit, but you’re not.
English
there's no single fix but the biology gives you levers before reaching for anything external.
diet breaks (2 weeks at maintenance) can partially reset leptin signaling. protein high enough to protect muscle. resistance training to defend BMR.
the goal isn't to push harder. it's to give the body enough safety signals to stop defending the weight.
sometimes that's enough. sometimes the hormonal environment needs a closer look, but that's the next step, not the first.
English

@HBH327788013139 the cortisol-mTOR antagonism doesn't need a title to be true.
English

A lot of people say their workouts aren’t working, but when you look closer, they are training on top of exhaustion, under-eating protein, skipping recovery, and expecting the body to adapt anyway.
It doesn’t work like that.
Your body needs a reason to build, but it also needs the resources to build.
That means enough protein, enough sleep, enough hydration, and enough recovery to turn training into progress instead of breakdown.
English