New @NEJM
For persistent atrial fibrillation, first-line pulsed field ablation (PFA) superior to medical therapy (AAD) in a randomized trial for preventing recurrent atrial arrhythmias @omwazninejm.org/doi/full/10.10…
🫀The failing right ventricle:
the most misunderstood chamber in critical care
For years, we focused on the left ventricle.
But in the ICU, the real killer is often the right ventricle.
->What is acute RV failure?
👉 Not just “weak contraction”
It’s a hemodynamic collapse syndrome:
RV dilation
↓ LV preload
↓ cardiac output
↑ venous congestion
➡️ → multi-organ failure
->The key pathophysiology (the vicious cycle)
1. ↑ Afterload (PE, ARDS, PH)
2. → RV dilation
3. → Septal shift → LV underfilling
4. → ↓ CO → hypotension
5. → ↓ RCA perfusion
6. → RV ischemia
👉 And the cycle accelerates
->The most important concept
👉 The RV does NOT tolerate pressure
Handles preload very well
Fails rapidly with afterload
➡️ Even small ↑ PVR → collapse
->Main causes you MUST think first
🔴 Pulmonary embolism
🔴 RV myocardial infarction
🔴 ARDS / mechanical ventilation
🔴 Decompensated pulmonary hypertension
🔴 Post-cardiac surgery
->Diagnosis is NOT obvious
There is no single sign.
👉 It requires suspicion + integration:
Clinical: congestion + hypoperfusion
ECG + biomarkers
POCUS (your best friend 🤓)
Hemodynamics
->Echo mindset (fast ICU approach)
👉 Don’t overcomplicate
Look for:
✔ RV dilation
✔ Septal shift (D-sign)
✔ TAPSE ↓
✔ Venous congestion
The real ICU mistake
❌ Treating RV failure like LV failure
->Management principles
👉 Think in 4 pillars:
1. Preload — “not too much, not too little”
Hypovolemic → small fluid
Congested → REMOVE fluid
👉 CVP is not a target, it’s a warning
2. Afterload, THE key target
✔ Treat PE
✔ Optimize ventilation
✔ Reduce PVR
👉 If afterload stays high → RV will fail
3. Contractility
Dobutamine
Milrinone
Levosimendan
👉 Choose based on context
4. Perfusion pressure
👉 Norepinephrine is your anchor
✔ Maintains coronary perfusion
✔ Supports RV function
->Ventilation: the silent killer
⚠️ Positive pressure = ↑ PVR
👉 Over-ventilate → worsen RV failure
->When nothing works
👉 Think early:
VA-ECMO
RV assist devices
🤓Key insight
This is NOT just a cardiac problem.
👉 It is a ventriculo–arterial coupling failure
When:
Ees / Ea ↓ → RV collapses
🤓Bottom line
✔ RV failure is preload dependent BUT afterload sensitive
✔ Small mistakes → rapid collapse
✔ Early recognition + physiology-based treatment saves lives
->Clinical mindset
👉 Don’t ask:
“Is the RV failing?”
👉 Ask:
“Why is the RV failing and, what is driving the afterload?”
📃Reference
Giannakoulas G. et al. European Heart Journal (2025) 00, 1–16 doi.org/10.1093/eurhea…
Cool use of digital twins: First we have seen for patients having successful catheter ablation of their heart arrhythmia (VT) by first working on their twin 3D replica before the patient.
@NEJM today nejm.org/doi/full/10.10…
Paper of the day: Fundamental Anatomy and its Impact on Clinical Practice: Bachmann's Bundle and Interatrial Conduction (Part I-III)
González-Casal D, Baranchuk A, Sánchez-Quintana D, Cabrera JA. JACC CR doi: 10.1016/j.jaccas.2026.107414.2026 Mar 16:107414
Working with the best
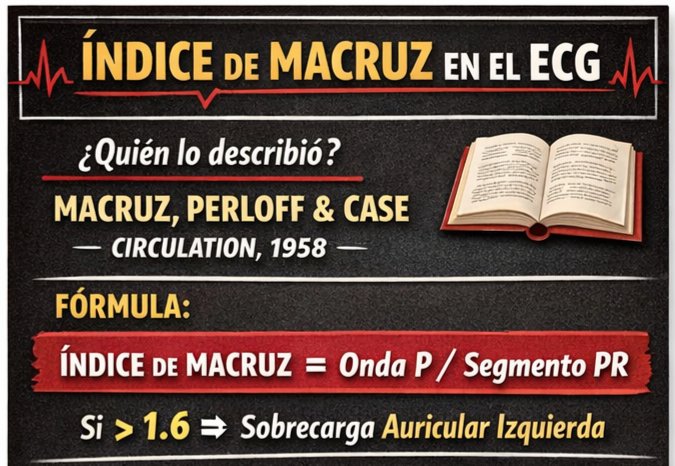
EKG: índice de Macruz. 🫀⚡️
🔶️Antes del ecocardiograma, el EKG ofrecía múltiples intentos de estimar la sobrecarga auricular izquierda. Uno de ellos es el Índice de Macruz, un parámetro poco mencionado hoy, pero con una utilidad rápida y fácil de implementar. ⚡️👍🏻
🔶️¿Qué es? Es la relación entre: duración de la onda P / duración del segmento PR [Índice de Macruz = P / segmento PR]. 🧮🧐
🔶️Valores de referencia:
▪️Normal ~1.0–1.6
▪️>1.6: sugiere sobrecarga AI.
🔶️Fisiopatología: cuando la AI se dilata o hipertrofia, su activación eléctrica se vuelve más prolongada, lo que aumenta la duración de la onda P. El segmento PR, que refleja principalmente la conducción a través del nodo AV, suele mantenerse relativamente constante. Por ello, cuando la onda P se prolonga sin un cambio proporcional en el PR, el cociente aumenta, elevando el Índice de Macruz. 📈⚡️
🔶️Interpretación clínica: un Índice de Macruz >1.6 puede sugerir crecimiento AI, especialmente en el contexto de enfermedad mitral.👨⚕️🔎
@JACCJournals@DrAJRestrepo@rafavidalperez@dgsomucla We had a very similar case a few months ago. Coronary angiography showed occlusion of the mid-LAD caused by the lead that was finally removed, leaving a residual fistula from LAD to RV opting for conservative management.
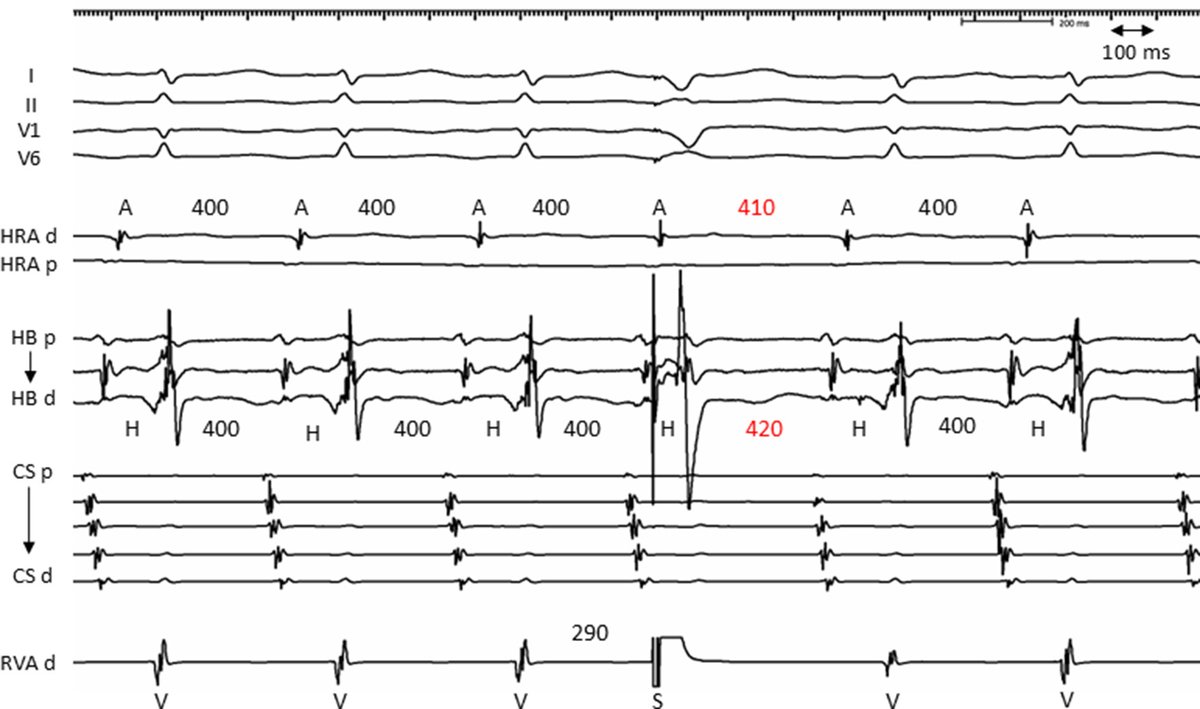
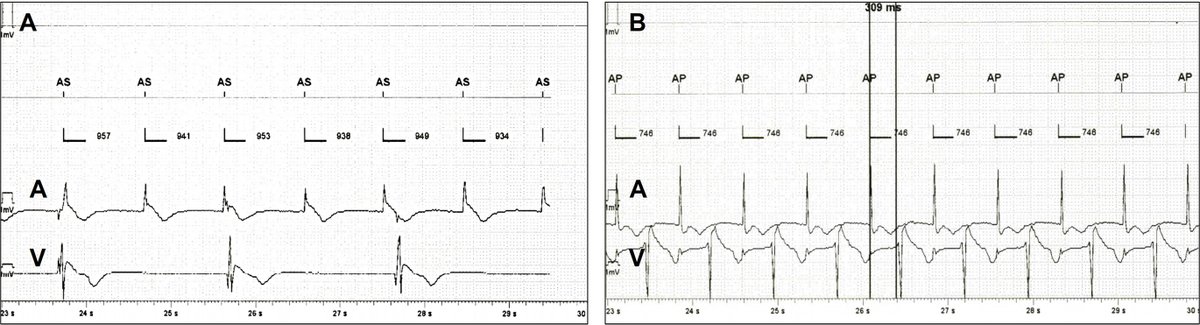
Rate-dependent transition from bradycardia-dependent atrioventricular block to inverse and conventional decremental conduction after transcatheter aortic valve replacement: A case report
heartrhythmcasereports.com/article/S2214-…