Sabitlenmiş Tweet
Michael Shusterman, MD
1.4K posts

Michael Shusterman, MD
@guildsman
Gastrointestinal Medical Oncologist @Perlmutter_CC, Associate Program Director @nyulisom_HemOnc. Tweets my own. #Meded
Mineola, NY Katılım Ağustos 2009
234 Takip Edilen926 Takipçiler
Michael Shusterman, MD retweetledi

Topline data from 55 ptnts in $IMRX Phase 2a trial of atebimetinib + mGnP demonstrates 17.3 mth median overall survival in 1L #PancreaticCancer - more than 2x standard of care. Full data to be presented on June 1st at the #ASCO2026. Learn more here: buff.ly/rcoOrk1

English
Michael Shusterman, MD retweetledi

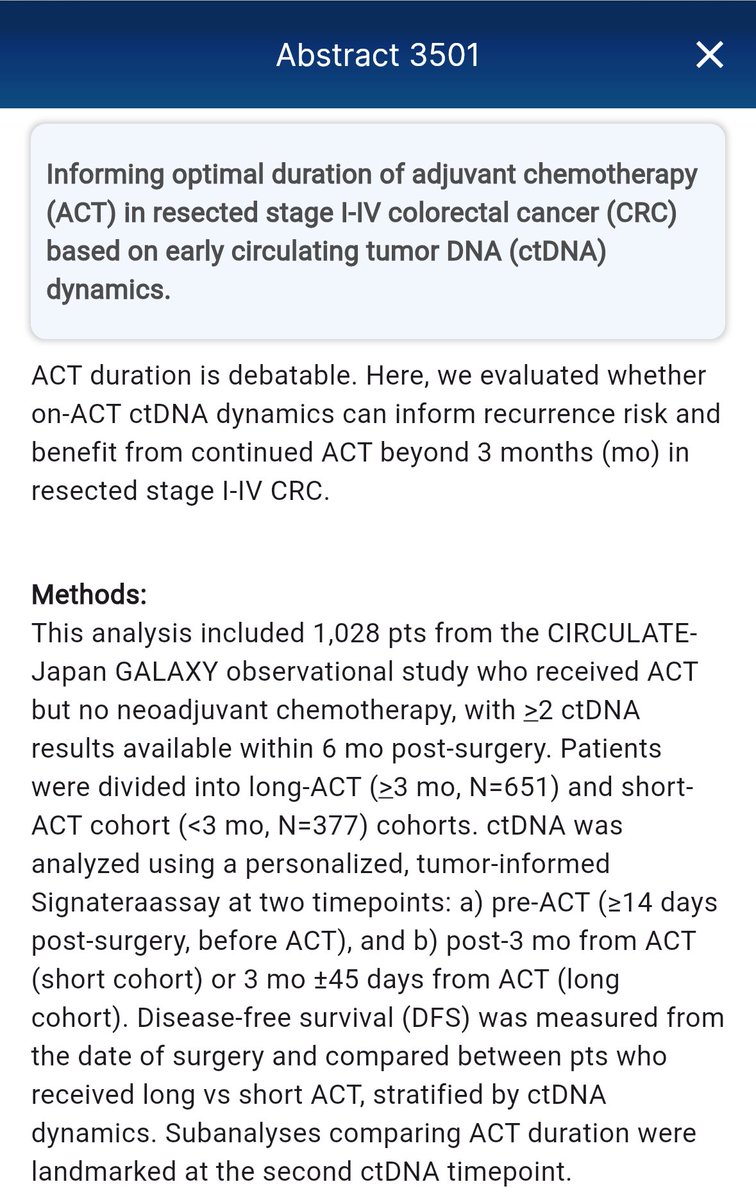
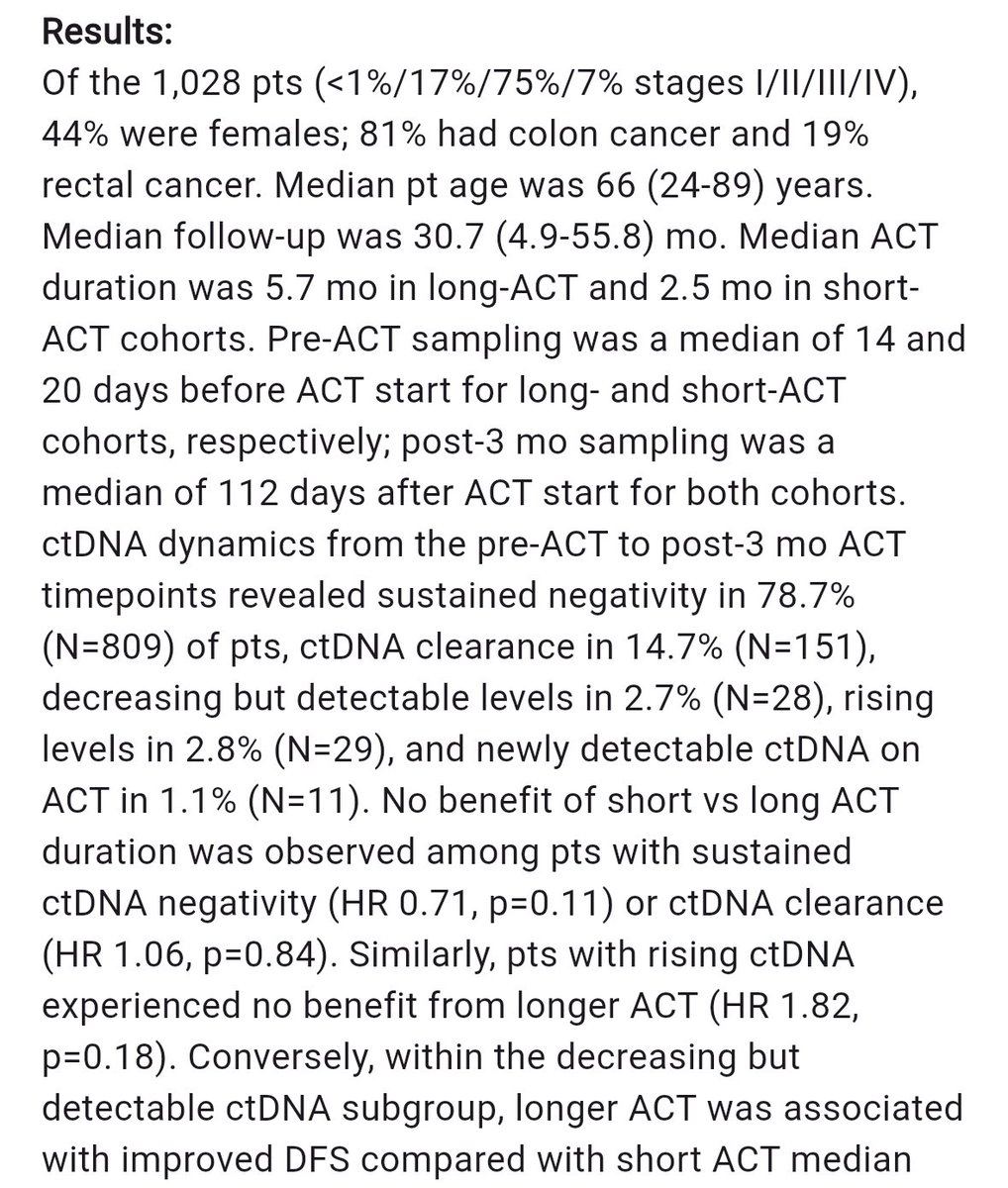
CIRCULATE-Japan GALAXY adj chemo (ACT) in StII/III CRC ➡️ 14.7% #ctDNA clearance, no benefit b/t short vs long ACT in this w/sustained #ctDNA neg or clearance, no benefit to longer ACT w/rising ctDNA but DFS benefit w/longer ACT in those #ctDNA+ and decreasing #ASCO26
@OncoAlert

Beverly Hills, CA 🇺🇸 English
Michael Shusterman, MD retweetledi
SBRT (50Gy/5fx, MR adaptive) in locally recurrent PDAC.
N=46 (7 w prior RT). 1 year LC 73%, median OS 19 mo.
Ablative RT = feasible, safe in locally recurrent setting & can confer long term dz control.
Great to see this data published - congrats @adapthyun & team! @OncoAlert
ASTRO@ASTRO_org
New in #practicalRO: Adaptive Salvage Stereotactic Radiation for Locoregional Recurrence of Pancreatic Adenocarcinoma After Surgery. #radonc tinyurl.com/prolakomy
English
Would be interested in combination therapy role in very high volume metastatic disease with risk of organ dysfunction (e.g. extensive liver involvement) as a debulking strategy.
Thor Halfdanarson@OncoThor
The AGITG CONTROL NETS is finally out in paper! Does the CAPTEM-PRRT combo perform better than CAPTEM in patients with pancreatic NETs? Well, there is more in this paper than that but let's focus on the pNETs. Bottom line: Complex trial, many moving parts, small cohort, does not and should not change practice. More thoughts: The study would suggest so with longer PFS in the PRRT/CAPTEM but the bigger question is how patients who got PRRT alone compare but that was not done here. Keep also in mind that the number of treated patients was very small. The PFS in the PRRT/CAPTEM group was 59.4 months which is very impressive (For PRRT alone reference, it was 20.7 months in OCLURANDOM and 24.5 months in COMPETE). There were only 2 patients (3%) among those who had PRRT who developed therapy-related myeloid dysplasia which is reassuring but also goes against what others have reported where the risk is as high as 10%. Will this change anything for me? Absolutely not as I would need larger studies to be convinced and also, I am not sure the therapy sequencing matters that much as long as you get all the effective therapy during the illness. But what this study does is to help revive the concept of chemo-PRRT and support the development of other trials looking at combining PRRT with systemic therapy and @AmanChauhanMD, I am looking at you now... 😉 sciencedirect.com/science/articl…
English
Michael Shusterman, MD retweetledi

🩺 THE 10 MOST IMPORTANT GI CANCER TRIALS OF #ASCO26
🌟 PLENARY & PRACTICE-CHANGERS
1️⃣ RASolute 302 (LBA5)
Daraxonrasib (RMC-6236) vs chemotherapy in metastatic pancreatic cancer
Can RAS finally become druggable in pancreatic cancer?
2️⃣ CIRCULATE (LBA3500)
ctDNA-guided adjuvant therapy in stage II colon cancer
Potentially the defining trial for escalation and de-escalation strategies.
3️⃣ EMERALD-3
Durvalumab + tremelimumab + lenvatinib + TACE in unresectable HCC
How aggressive should frontline liver cancer therapy become?
🧬 COLORECTAL CANCER PRECISION ERA
4️⃣ BREAKWATER Cohort 3 (LBA3503)
Encorafenib + cetuximab + FOLFIRI in BRAF V600E mCRC
Important real-world sequencing data beyond oxaliplatin-based therapy.
5️⃣ SWOG S2107
Sequencing optimization in BRAF V600E metastatic CRC
A major unmet-need clinical question.
6️⃣ STELLAR Update
Long-term survival update for TNT in rectal cancer
Do pCR gains translate into durable survival benefit?
🎯 GASTRIC, GEJ & RARE GI SUBTYPES
7️⃣ HERIZON-GEA-01 (4010)
Zanidatamab-based frontline therapy in HER2+ gastric/GEJ cancer
Could bispecific HER2 targeting redefine frontline care?
8️⃣ KEYNOTE-811 Mature OS
Final long-term OS update for pembrolizumab + trastuzumab + chemotherapy
Clinicians have been waiting for these mature survival curves.
9️⃣ ATTRACTION-6 Update
Checkpoint inhibitor strategies in advanced gastroesophageal cancers
The IO sequencing debate continues.
🔟 Bezuclastinib + Sunitinib (11500)
Phase III data in advanced GIST
A key resistance-targeting strategy in rare GI oncology.
Which GI abstract will change your clinic most?
#GIOnc #OncTwitter #ASCO26 #PanCan #ColorectalCancer #MedTwitter @ASCO @myesmo @esmo_open @OncoAlert

Dr Rishabh Jain@DrRishabhOnco
🚨 THE 15 MOST IMPORTANT TRIALS OF #ASCO26 May 29 - June 2 | Chicago Which trial are you watching most closely? 🌟 PLENARY GAME-CHANGERS 1️⃣ PROTEUS Perioperative apalutamide + ADT in high-risk localized prostate cancer 2️⃣ LIBRETTO-432 Adjuvant selpercatinib in RET+ NSCLC 3️⃣ HARMONi-6 Ivonescimab + chemo vs tislelizumab + chemo in squamous NSCLC 4️⃣ RASolute 302 Daraxonrasib (RMC-6236) in metastatic pancreatic cancer 5️⃣ SARC041 Abemaciclib in dedifferentiated liposarcoma ⚡ FRONTLINE & PERIOPERATIVE SHIFTS 6️⃣ KEYNOTE-B15 / EV-304 EV + pembrolizumab vs chemo in MIBC 7️⃣ LITESPARK-022 Pembrolizumab + belzutifan in adjuvant ccRCC 8️⃣ AMBITION Paclitaxel/bevacizumab ± atezolizumab in HR+ breast cancer 9️⃣ NeoADAURA Neoadjuvant osimertinib in EGFR+ NSCLC 🔟 A-DREAM ADT interruption strategies in mCSPC 🧬 PRECISION, ADCs & NEXT-GEN IMMUNOLOGY 1️⃣1️⃣ DESTINY-Breast06 T-DXd expands into HER2-ultralow disease 1️⃣2️⃣ CROWN (7-year update) Lorlatinib durability in ALK+ NSCLC 1️⃣3️⃣ DeLLphi-312 Tarlatamab in frontline SCLC 1️⃣4️⃣ COMMIT Atezolizumab + FOLFOX/Bev in MSI-H mCRC 1️⃣5️⃣ IMvigor011 ctDNA-guided adjuvant atezolizumab in bladder cancer #OncoTwitter #MedTwitter #ASCO26 #CancerResearch @OncoAlert @ASCO @JCOPO_ASCO @OncBrothers
English
Michael Shusterman, MD retweetledi

Evaluation and Treatment of Iron Deficiency for the Practicing Oncologist | JCO Oncology Practice ascopubs.org/doi/pdf/10.120… @JCOOP_ASCO @ASCO @OncoAlert one of the most common consults in General HemOnc Clinics


English
Michael Shusterman, MD retweetledi

👏🏽 ELEGANT paper on mechanisms of resistance to tricomplex RAS inhibitors (eg, daraxonrasib) published in @CellCellPress!
THREE major pathways observed:
1⃣ RAS Y64 mutations (weaken daraxonrasib indole ring with weaker KRAS tricomplex formation)
2⃣ RAS Y71 mutations (allosteric effect ▶️native RAS-RAF interaction favored over tri-complex)
3⃣ Class III BRAF mutants (RAF dimerization repositions cysteine-rich domain ▶️ intensifies native KRAS binding ▶️ harder for tricomplexes to displace
A MAIN insight [for me] is that cancer cells, when faced with intense selection pressures from potent targeted therapies, will often take the path of LEAST resistance!
⭐️Authors show [Figure 1] that there is virtually NO bypass signaling through ERBB or MET family.
⭐️Almost ALL resistance is mediated through alterations in native MAPK pathways, which makes sense (path of least resistance)
EXCELLENT one to bookmark and return to:
👉🏽 cell.com/cell/fulltext/…
@lcsmchat @OncoAlert @KRASKickers @OncogeneCancer @OncLive @Lung_Cancers @MedwatchKate @YoungLungCancer
English
@TimothyJBrownMD Agreed regarding type of gastrectomy varied. Also some patients can tolerate chemotherapy but have underlying neuropathy and taxane and platinum can be very, very challenging. I using cryotherapy and still can be hit or miss with neurologic complications.
English

@guildsman Bigger q- if someone is too frail for DFLOT, are they realistic candidates for gastrectomy?
English
Also for more frail patients, can we use FOLFOX Durvalumab?
Tim Brown, MD MSCE@TimothyJBrownMD
Completion of all planned perioperative therapy was associated with best outcomes in MATTERHORN 🗻🗻. Intuitive but an important signal when counseling patients- dose reduce if you must but try to complete. @GIMedOnc @UGrewalMD @TheGutOncLab asco.org/abstracts-pres…
English
Michael Shusterman, MD retweetledi

Until now, physicians using AI in clinic had to assemble the patient’s context themselves. Allergies, comorbidities, medications, prior procedures, copy-pasted in from the chart.
Today we’re announcing a partnership with @CedarsSinai. OpenEvidence now works directly inside Epic, drawing on the patient’s full record and interpreting the medical literature through the lens of that specific patient.
Cedars-Sinai is the first academic health system to deploy patient-aware clinical intelligence at enterprise scale. The clinician asks a complex question in natural language. The answer reflects both the best available evidence and the patient in front of them.
Patient data is never stored after the clinical session or used for any other purpose.

English
Michael Shusterman, MD retweetledi

I am not loving this trend of AI generated infographic explanation of pivotal clinical trial data. Many of them are straight up wrong as they aren’t peer reviewed or even created by an expert in that cancer type. Be CAREFUL when using these to learn about data and look at the source. #bcsm #breastcancer
English
Michael Shusterman, MD retweetledi

Managing toxicity is hard.
It is part science, part judgment, and part art. And it is not always fully spelled out in the package insert.
In advanced GI cancers, we spend a lot of time talking about the next drug, the next target, the next trial.
But for many patients, the most important question is more practical:
Can we deliver effective therapy in a way they can actually tolerate?
Dose modifications. Schedule adjustments. Quality of life.
This is the real world of oncology.
Grateful to publish this review with @GutOncLab, @UGrewalMD @TimothyJBrownMD @guildsman on optimizing systemic therapy for advanced GI cancers.
Personalized dosing is not “less aggressive” care.
Done thoughtfully, it is often better oncology.
@OncoAlert @Onco_Nexus
clinical-colorectal-cancer.com/article/S1533-…
English
An amazing team of authors from @TheGutOncLab and @Perlmutter_CC came together to discuss real world doses, toxicity management, and optimizing regimens in GI Oncology. First author Dr. Sabrina Bulancea will be an oncology star, congrats on starting fellowship soon! @OncBrothers
Nicholas Hornstein@GIMedOnc
Managing toxicity is hard. It is part science, part judgment, and part art. And it is not always fully spelled out in the package insert. In advanced GI cancers, we spend a lot of time talking about the next drug, the next target, the next trial. But for many patients, the most important question is more practical: Can we deliver effective therapy in a way they can actually tolerate? Dose modifications. Schedule adjustments. Quality of life. This is the real world of oncology. Grateful to publish this review with @GutOncLab, @UGrewalMD @TimothyJBrownMD @guildsman on optimizing systemic therapy for advanced GI cancers. Personalized dosing is not “less aggressive” care. Done thoughtfully, it is often better oncology. @OncoAlert @Onco_Nexus clinical-colorectal-cancer.com/article/S1533-…
English
Really important, current ctDNA does not have high sensitivity for pancreatic cancer. Something unique in shed rates.
Syed A. Ahmad@SyedAAhmad5
Invited commentary on: “Post-surgical ctDNA as a prognostic biomarker for relapse of resected pancreatic ductal adenocarcinoma” sciencedirect.com/science/articl…
English
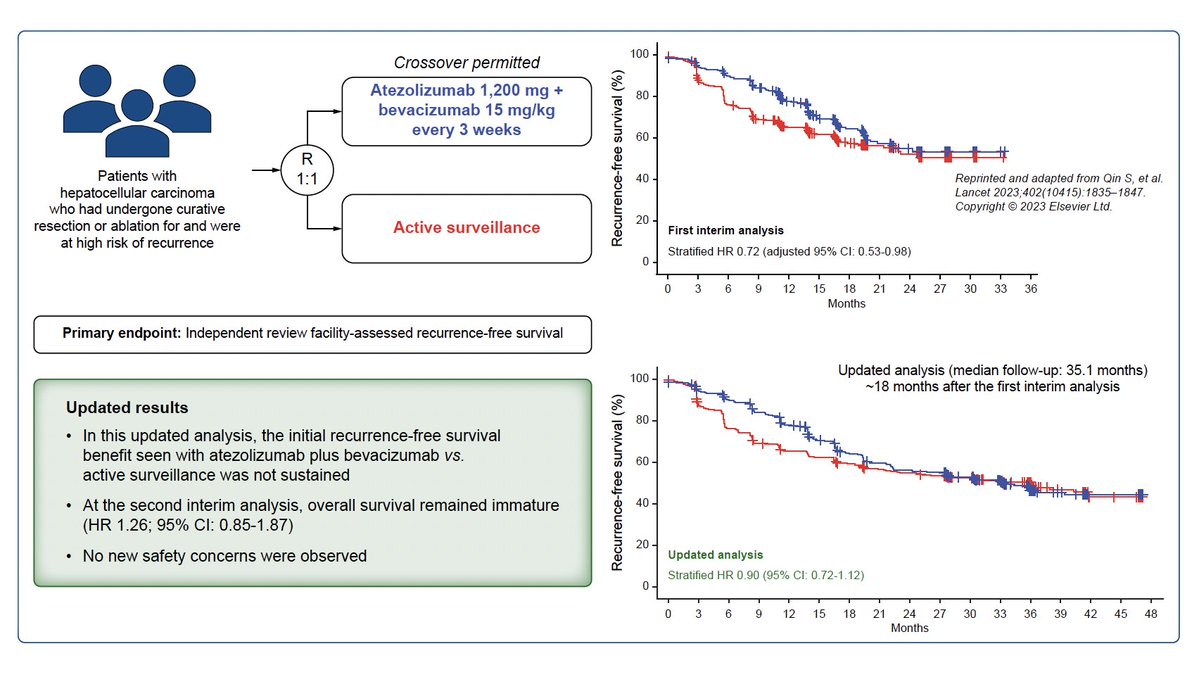
Michael Shusterman, MD retweetledi

Updated data from IMbrave050: Adjuvant atezolizumab plus bevacizumab for high-risk hepatocellular carcinoma
@JHepatology
doi.org/10.1016/j.jhep…
👉Disappointing, we need to do better...
@myESMO @EASLedu @ILCAnews
English
Michael Shusterman, MD retweetledi

🟡Transforming perioperative treatment of gastro-oesophageal adenocarcinoma
✅state-of-the-art perioperative management
👉nature.com/articles/s4157…
#cancer #oncology #MedX #gastric @LizzySmyth1 @KoheiShitara @DrHongchengZhu @YJanjigianMD


English
Michael Shusterman, MD retweetledi

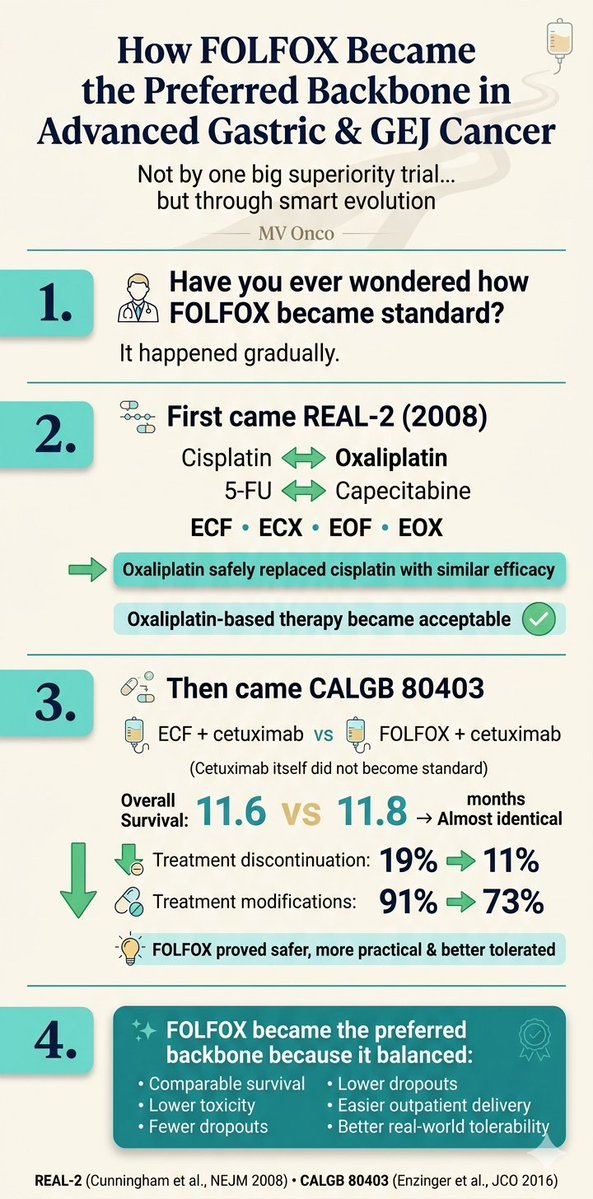
How did FOLFOX become the preferred backbone in advanced gastric & GEJ cancer?
• Not through one dramatic superiority trial
• REAL-2 showed oxaliplatin could replace cisplatin with similar efficacy
• Oxaliplatin-based therapy then became acceptable
• CALGB 80403 later showed similar survival with FOLFOX
• But importantly: lower treatment discontinuation and fewer treatment modifications
• Cetuximab itself did not become standard — the FOLFOX backbone did
Sometimes a regimen becomes standard because it is:
• easier to deliver
• better tolerated
• more practical in real-world oncology
#GastricCancer #GIOncology #FOLFOX #Oncology #MedicalOncology #MVOnco
English
Michael Shusterman, MD retweetledi

1/n
Daraxonrasib (RMC-6236), the first-in-human oral 💊RAS(ON) multi-selective tri-complex inhibitor, in previously treated RAS-mutated pancreatic cancer phase I/II study is now published in the New England Journal of Medicine @NEJM
A novel💡 way to shut down ⚔️RAS, one of the most important oncogenic drivers in cancer that had long been considered “undruggable.”
🔗nejm.org/doi/full/10.10…
Shout out to Brian Wolpin, @CentralParkWMD @GarridoLagunaMD @AlexSpiraMDPhD @salmanpunekar @MeredithPelster @bherzbergmd Nilo Azad Aparna Hegde @DavidHongMD and the whole team who dedicated to this study. @EileenMOReilly
#HBP #HumansBeyondPatients
Manhattan, NY 🇺🇸 English
We have been using prophylactic antibiotics and steroid creams. It seems to work for some. But the mucositis I have not figured out a solution to. Also some of the rash is totally refractory. Still can get most patients through and when it works, it’s fantastic.
Udhayvir Grewal@UGrewalMD
Phase 1/2 data for Daraxonrasib are now published in @NEJM - Patients with pretreated PDAC harboring KRAS, NRAS, or HRAS mutations at codons 12, 13, or 61- received Daraxonrasib once daily in 21-day cycles at doses ranging from 10 mg to 400 mg. MTD was not reached, 400 mg was maximum administered dose. 🚨📛Important to highlight the toxicities here (300 mg, n=83)- rash (in 90%), stomatitis or mucositis (in 54%), diarrhea (in 52%), and nausea (in 39%)--Grade 3 or higher occurred in 34% of the patients. Dose modifications:48% (dose interruption: 43% and dose reduction: 30%). However, no patients discontinued treatment due to AEs. 📈📊Now looking at efficacy- at a median follow-up of 17 months, mPFS=8.5 months, mOS=13.1 months. ORR 29% with median time until objective response= 2.6 months and duration of response= 8.2 months. 👏🔥 💯💯Overall impressive data for efficacy but it is obvious that this comes at a price, i.e., toxicity! But this is true for any drug, especially TKIs- rash, GI tox, etc are not new toxicities with TKIs. I bet as our experience with these agents grows, we will find ways to minimize these and preserve QoL as our patients continue to benefit from these game changing novel agents. This sets the stage for whats coming at #ASCO26 nejm.org/doi/full/10.10…
English
Michael Shusterman, MD retweetledi

Merck announced negative results for KEYNOTE-975:
Pembrolizumab + dCRT did not improve EFS in locally advanced esophageal carcinoma.
@OncoAlert

English