@Dr_GuyRozen Thanks Guy. I wonder though, if there would still be an increased risk placing a second lead at more experienced centers or more experienced operators?
@narrowQRS@EM_RESUS@PPodrid@ecgrhythms Josh what would you do with slower atypical flutters? Say 150-200? Do you skip anticoagulant and ablate w/o tee then?
@EM_RESUS@PPodrid@ecgrhythms In atrial flutter proper, there is always electrical activity occurring, so there is not an isoelectric segment between flutter waves. In focal atrial tach, there usually is a flat section between p waves, as is the case here. Of course there are exceptions in both directions.2/2
@javadm20 I would introduce the ablation catheter back in carefully through the correct lumen before it is taken out of the groin as that segment may break off in the fem vein
@AveragingBogey I had a patient w AV block from sarcoidosis. No antegrade conduction but slow retrograde conduction. During dual chamber pacing he’d spontaneously go into slow PMTs.
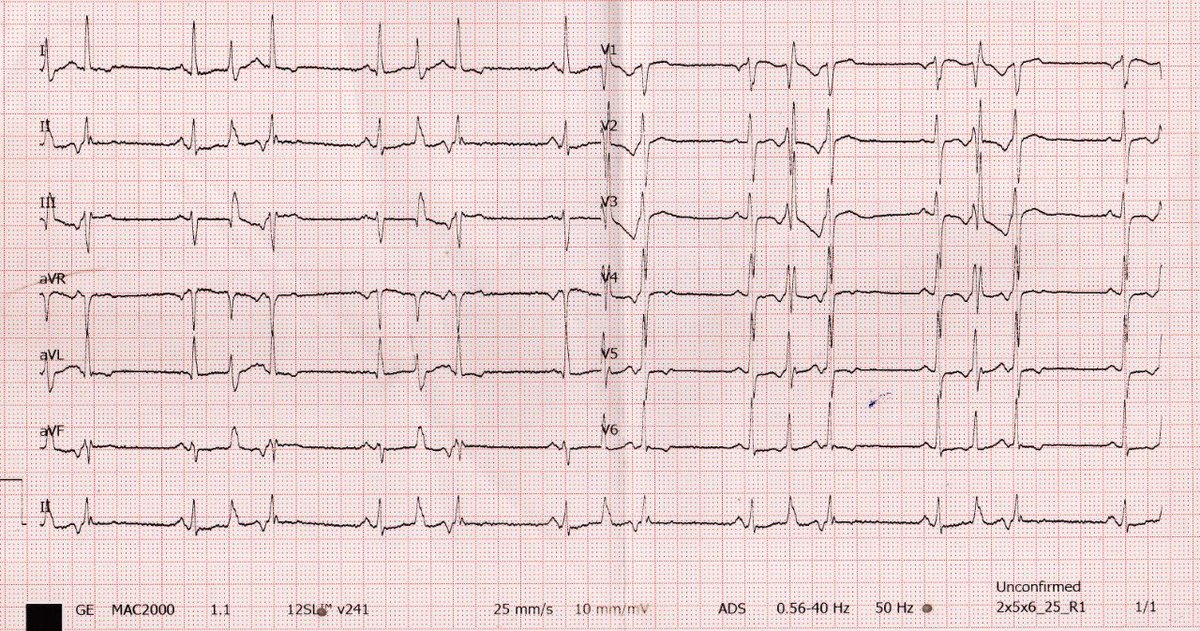
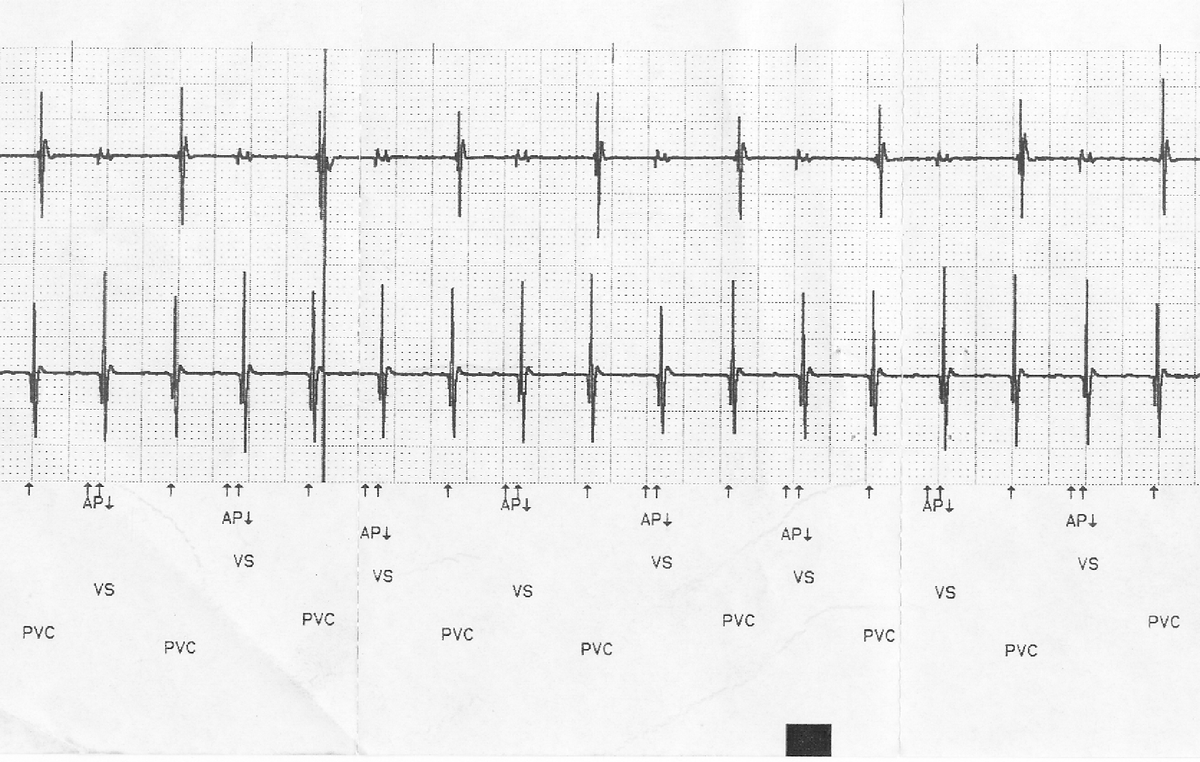
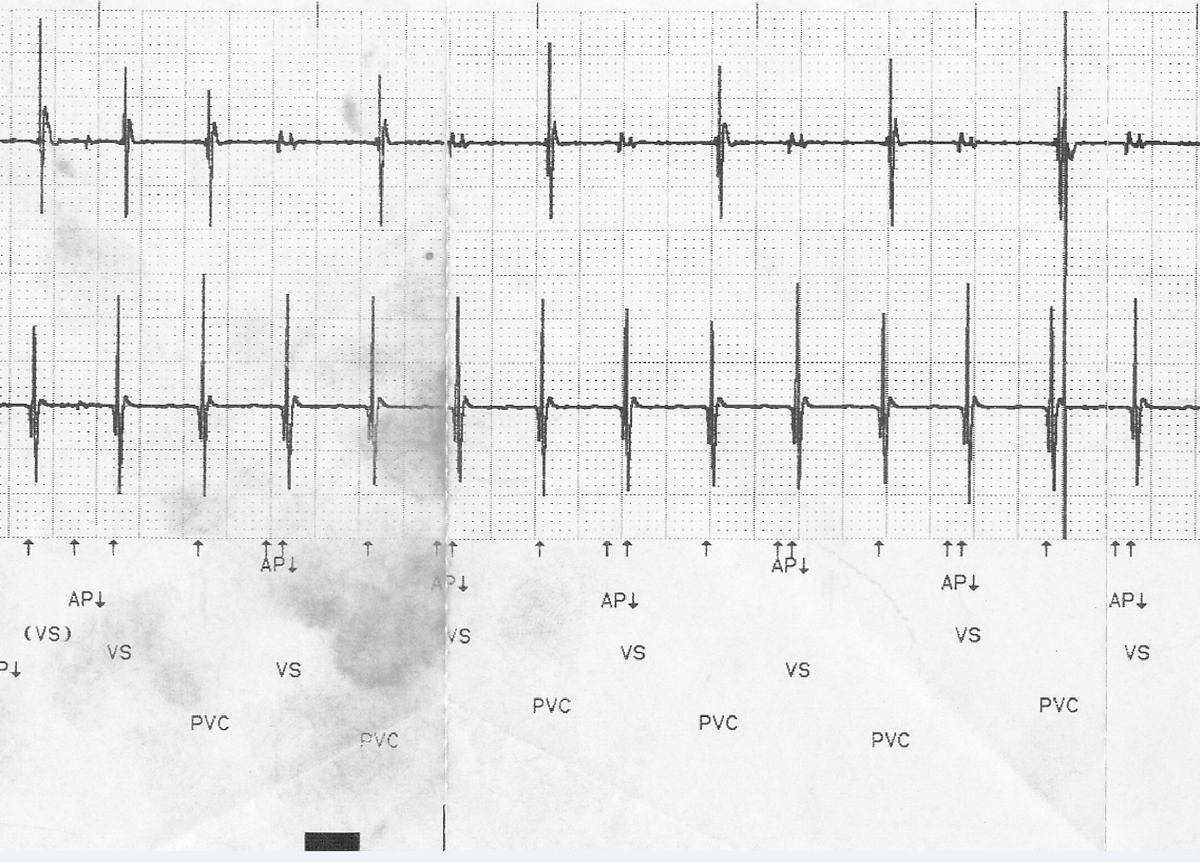
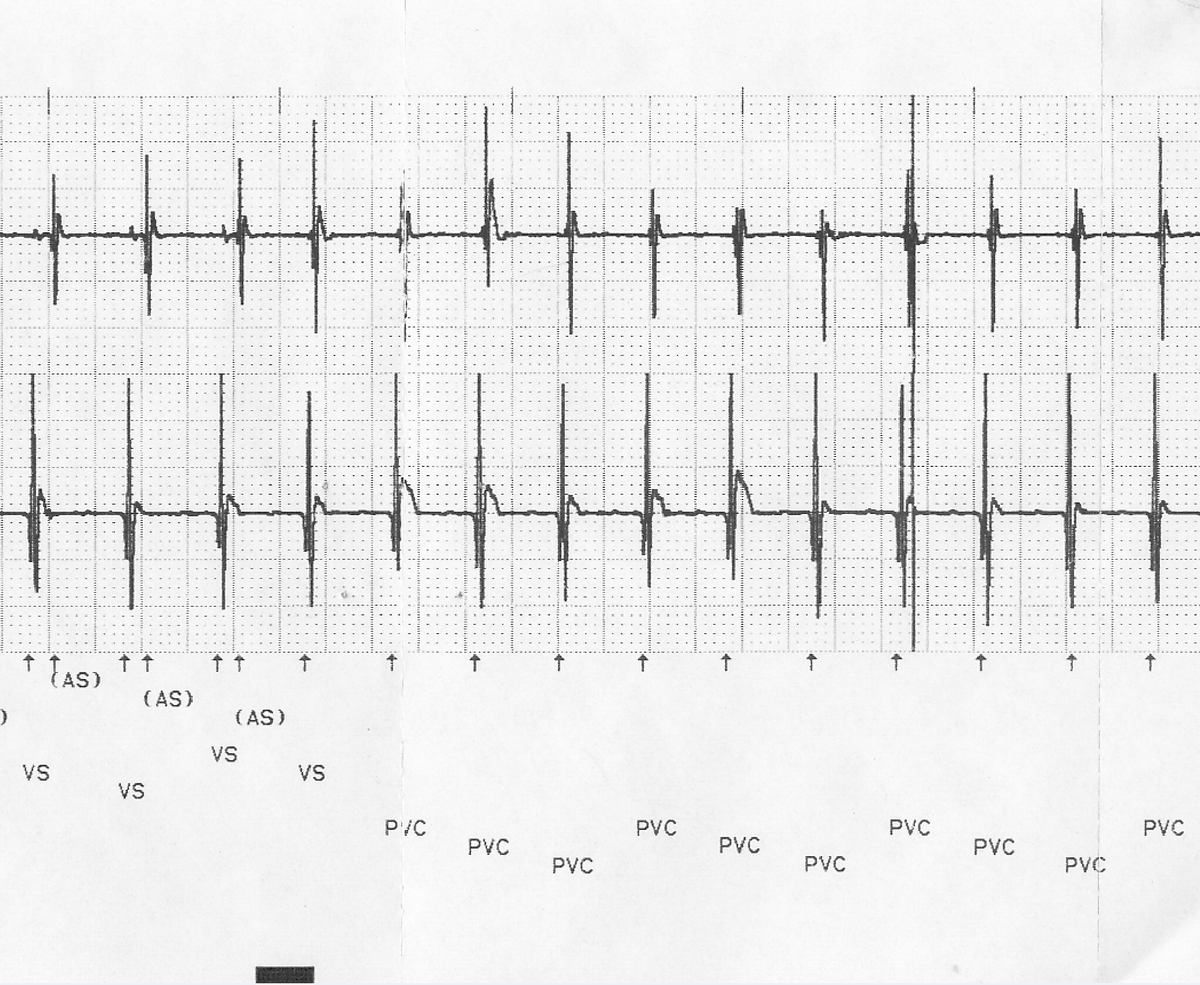
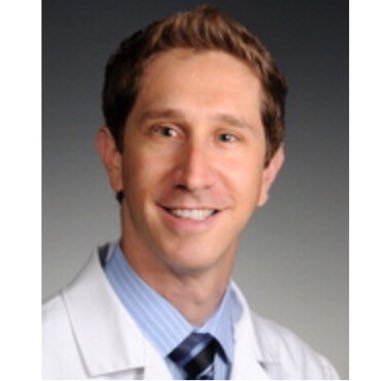
#EPeeps recent CRT implant, hook up device and this tachy within 3-5 first few AV paced beats. Reproducibly terminates immediately w ODO programming indicating PMT. Ever seen PMT initiate seemingly spontaneously? RA threshold 0.5V@0.4ms, confirmed in AAI mode.
@javadm20@narrowQRS@rdschaller@SergioPinski@SchakrabartiEP If no effusion/he’s stable don’t do anything until noac is held for a few days. Get tte right away and ct if possible to delineate lead location better. If truly emergent could give kcentra/andaxanet.
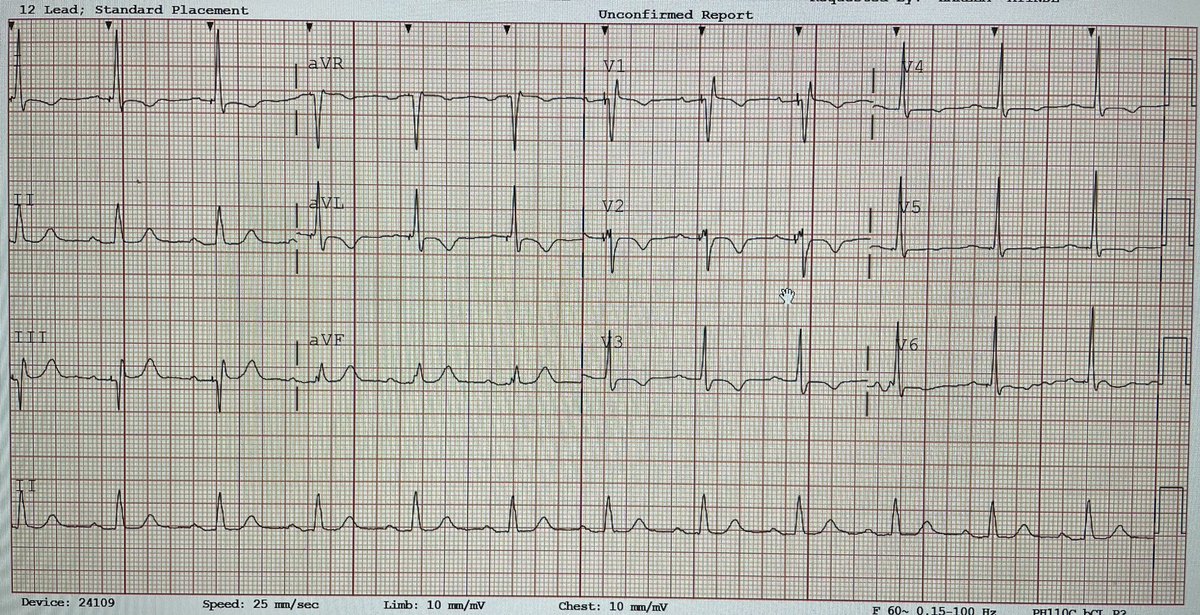
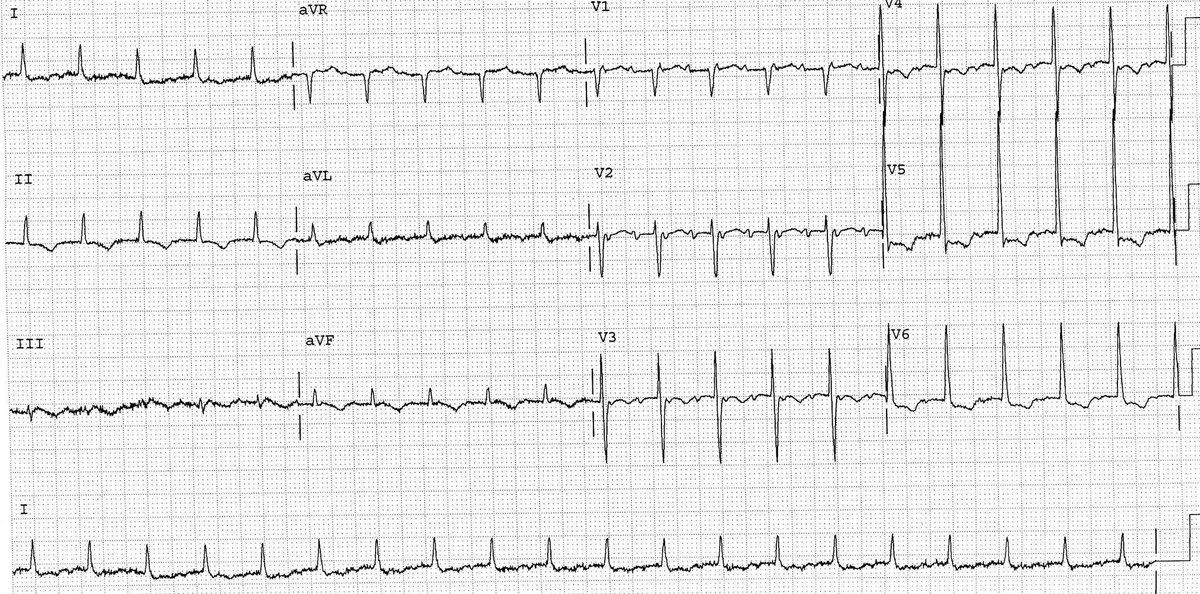
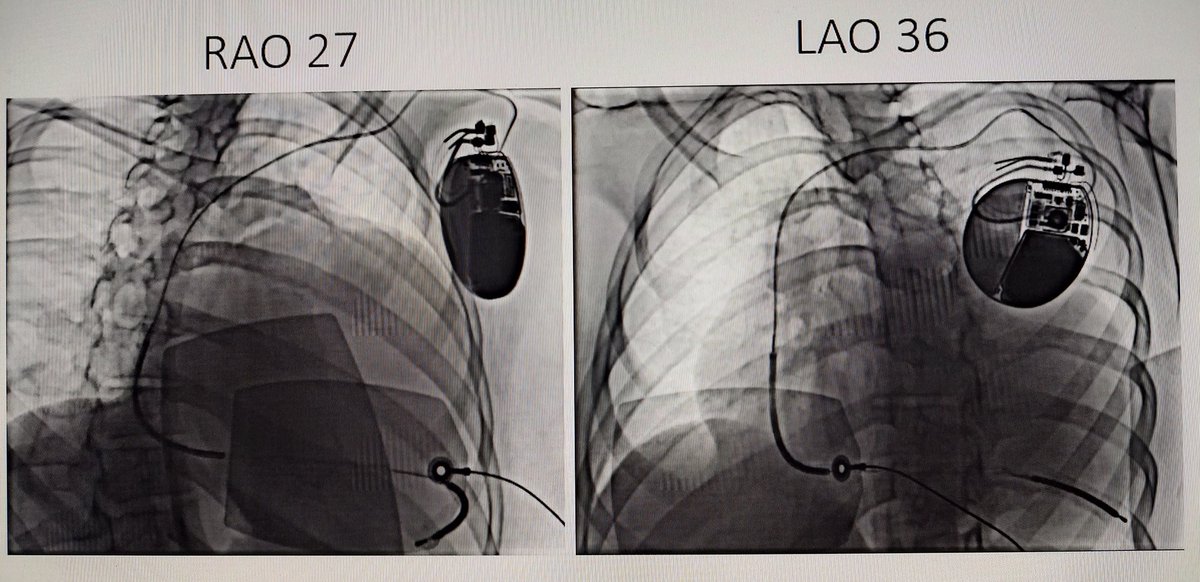
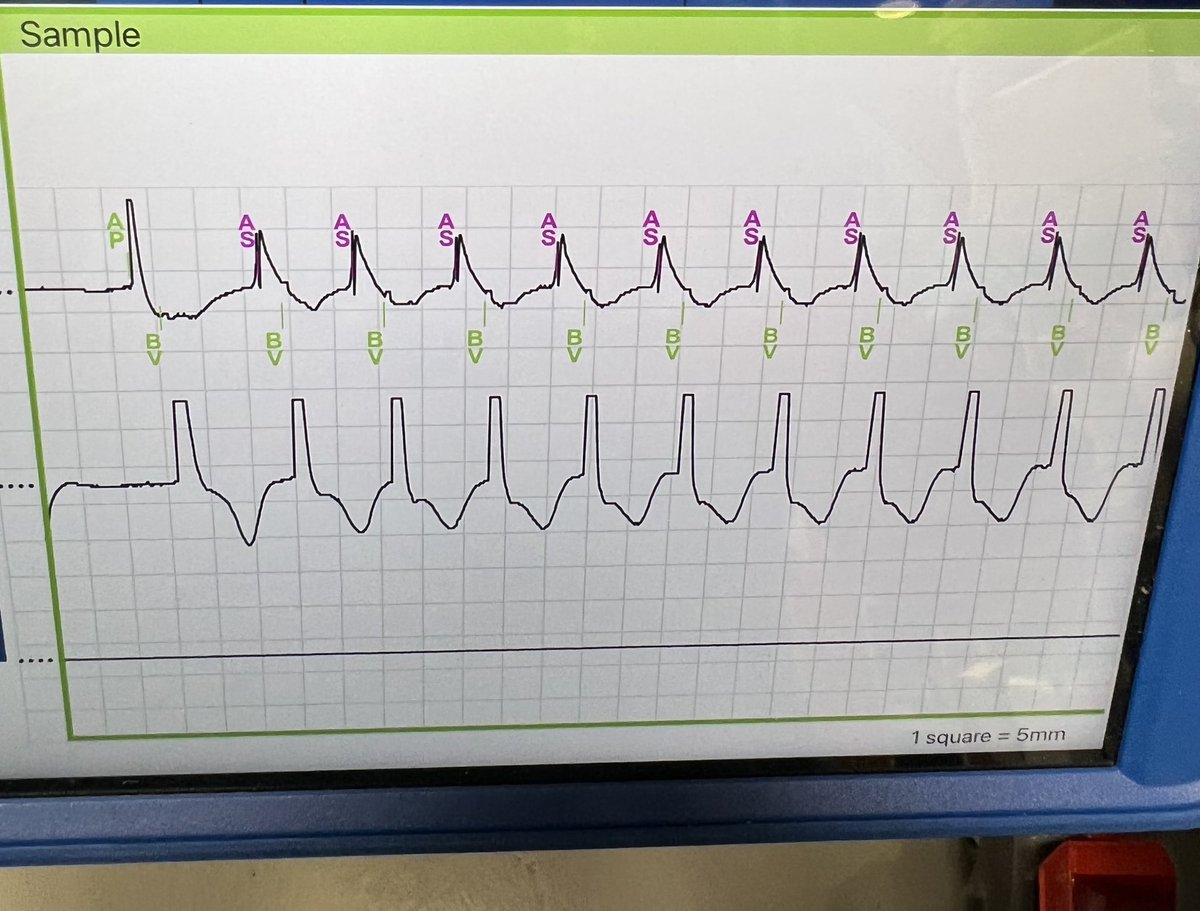
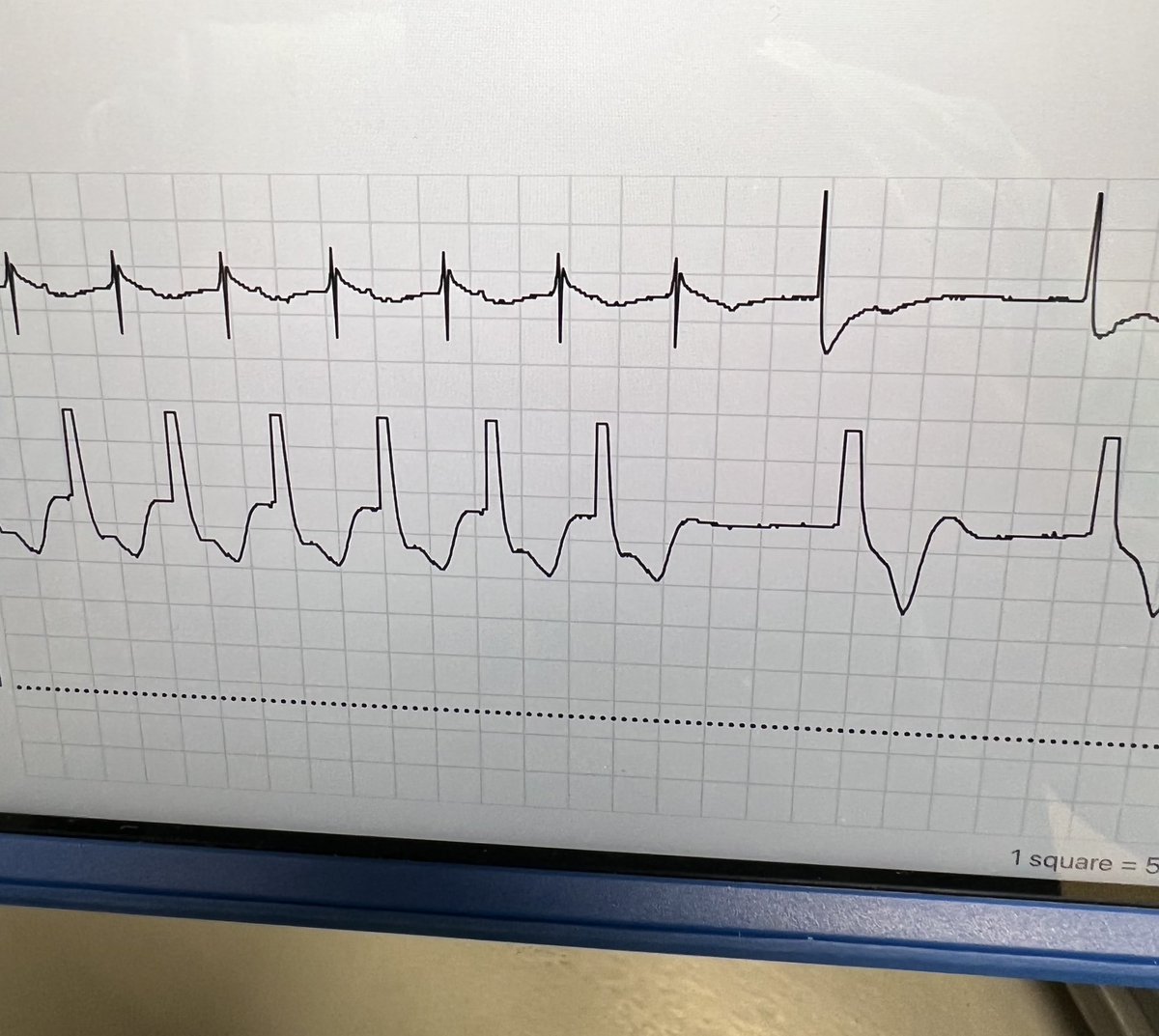
Today’s case! ICD was implanted one month ago! On apixaban 5mg/bid due to hx of unprovoked DVT! p/w loss of capture & sensing drop! RAO view 🤦🏻♂️!#Epeeps
@EJSMD Some very directed training: vasc surg mostly, plastics (a little) and I would’ve love to spend more time in the OR watching open hearts (not sure I would’ve needed to actually do much but learning anatomy and observing)
Curious—
Is there another non-surgical sub-specialty that does as much surgery than EP?
Should a component of formal surgical training be part of #EPeeps education?
@StevenZweibel I’ve seen it- similar presentation (swelling/discharge on both sides). Skin testing using Abbott’s kit was negative for all components. We had used a tyrx pouch during both implants initially, so ended up doing an implant w/o the pouch and were successful.
(1/2) Very promising technology in development for ablation of difficult to reach VT SOOs. Focused electrical field (FEF) delivers deeper lesions using just a standard RF generator
Ex-vivo:50Wx2 min, CF 15 g, NS 30ml/min -> 1.45 cm deep lesion #EPeeps@JonMelman@JRWinterfield
@narrowQRS@Dr_Nazarian_EP@jeffrey_vinocur@5Stabbies That’s interesting Josh. What I don’t understand is why every low amplitude atrial EGM actually starts before the V? If it starts earlier why is it blanked ?
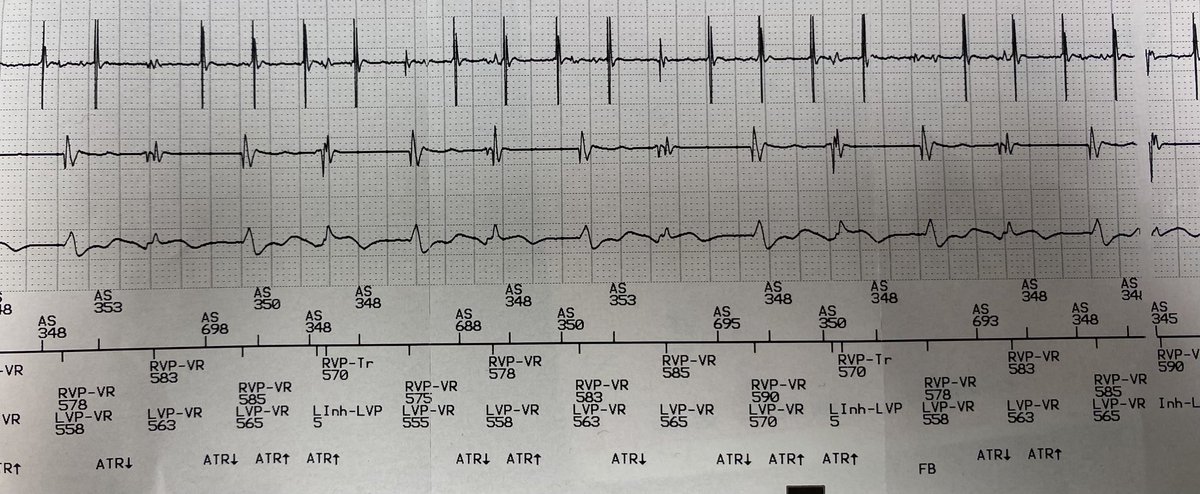
@Dr_Nazarian_EP@jeffrey_vinocur@5Stabbies Here's just one example of many I've seen.
This one initially makes the SVT look like VT with 2:1 VA relationship. But actually it's always a 1:1 SVT where every other atrial egm is sometimes erased by the pacer due to channel blanking/filtering during simultaneous AP events.
@skarim01@EPeeps_Bot@Drdevignair@SalmaBakshMD@aartisdalal@Nishaki1@KhaziRashad@drimdadahmed The "long" internal isn't that long (~100 bpm). And K+ 3.2 isn't dramatic. And can't pinpoint a specific cause that won't happen again. And can't rule out an underlying predisposition.
Would implant secondary prevention ICD. Could do MRI, but low yield. Consider genetic testing.