
Waleed Sneij
252 posts
Today our team was out in Historic Downtown St. Augustine conducting a large-scale larvicide treatment as part of our ongoing mosquito control efforts.
In just 7 hours, they treated approximately 1,000 storm drains using long-lasting products designed to control mosquitoes.
English
@nickmmark @PulmCrit Good point about POC EEG monitoring. But how about the data that succinylcholine is dangerous in status? What is that based on? (This is coming from a person who uses roc almost exclusively)
English

@kastlegacy @PulmCrit There is point of care EEG now. It’s a game changer in status and especially NCSE. We have it in all our EDs and ICUs. In fact it was shown in the episode! (It even says “status epilepticus” on the screen!)
It makes Abott’s decision making re Sux vs Rocc even more indefensible!


English
Weird medical decision making in the final episode of the Pitt
1. Using diazepam instead of lorazepam in status epilepticus. The latter is probably superior. Probably should have used more mag too.
2. They delayed intubation until she was clearly in status. I get waiting a minute to see if the mag works but giving multiple second line meds before deciding to take the airway is not a great move imho.
3. This is the big one. Using succinylcholine to intubate a seizing woman with eclampsia —> major risk for provoking hyperkalemia and cardiac arrest, which is exactly what happened! The rationale was “we need a neuro exam after”. Dude first of all you are gonna use an EEG to titrate anti-seizure meds (they showed this). Second you can just reverse roccuronium with suggamadex. That’s way more reliable than *hoping* the dangerous drug you gave wears off (in a patient with renal and liver injury no less)!
4. I could quibble about transfusions too. Rapid infusing blood when her Hb was 7 is wrong, though she was actively bleeding so 🤷 . Platelets should be transfused to >50k not necessarily higher. They didn’t give FFP for some reason, which is not good.
5. The depiction of the resuscitative hysterotomy was realistic but not having OBs there? Pretty unlikely. If there are OBs anywhere in the building you better believe they will be at the bedside of the eclamptic seizure code! (When I’ve done resuscitative hysterotomy IRL, lack of OBs was not a problem!) From a realism perspective this is not as bad as ER docs declaring brain death within a few hours of an overdose (season 1) but really felt unrealistic in a big urban academic hospital.

English
@PulmCrit @nickmmark What's your data about hyperkalemia and status epilepticus / eclampsia? Roccuronium reversal is often not available, and EEG monitoring setup takes a lot of time no matter where you are.
English
@nickmmark agree.
the whole roc-vs-succ debate in status epilepticus predates sugammadex. I’ve always been a roc fan here, but now that we have sugammadex that clinches the debate. 1st priority = airway control without killing the patient. Then give sugammadex and get back neuro exam.
English

Our team completed the Training Day for this season, preparing to install large-scale mosquito trap networks. 🦟
🏨 Hotels, restaurants, outdoor venues in France—our #MosquitoControl service is available!
✅ Service in France, expanding soon! Interested in partnering with us?




English
@budfraziershat @ThinkingCC what's the big deal about this block?
English

@ThinkingCC It isn’t the job of an ED doc to do Stellate block on a nursing home patient. Period. No armchair quarterbacking necessary.
English

Disappointed by the comments here. While an element of truth, most don’t come from a kind place, and it isn’t the job of an ED doc to right inappropriate societal patterns. Walk a mile in those shoes. Very easy to armchair quarterback.
Josh Guttman@drjgutt
1/ Wild cardiac arrest with #POCUS playing a major role An elderly male was sent from the nursing home in cardiac arrest. Per the prehospital report that we got, the patient was in vfib and refractory to 5 defib attempts. The patient got amio as well as several doses of epi.
English
@KernalGobz @ross_prager @NTFabiano @katiewiskar @NephroP @ThinkingCC @ArgaizR @kwadwo777 @KwadCast Interesting you broke it up into segements of 4 hrs pre and post. I've come to learn (from experience) that 4hrs (minimum) is the magic cutoff in terms of being able to function on your shift.
English

@ross_prager @NTFabiano @katiewiskar @NephroP @ThinkingCC @ArgaizR @kwadwo777 @KwadCast I'm reading this whilst there is a lull in my night shift. I think the most important part is the sleep. I try make sure I sleep for hours pre shift and then 4 hours minimum post shift. Just too try maintain my weekly average sleep at around 8 hours/ daily
English

Night shifts are associated with a higher risk of death ☠️👇
Here are some evidence based approaches to maintaining healthy while working shifts. A 🧵
(1/x)
English
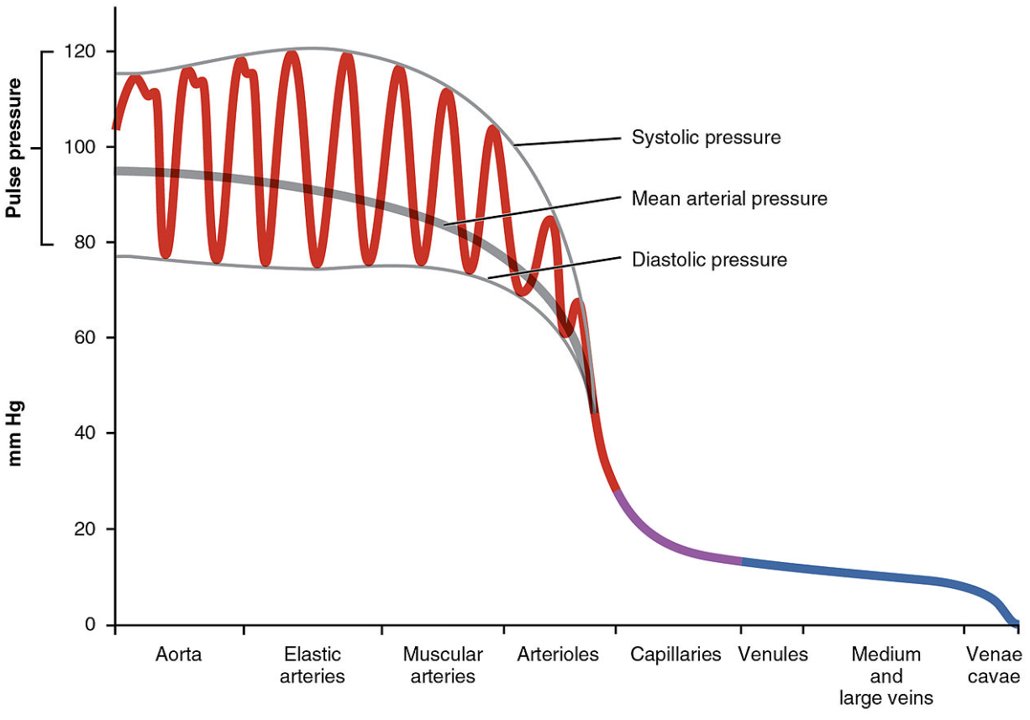
@ross_prager anaphylactic shock as ddx under narrow pulse pressure?
English
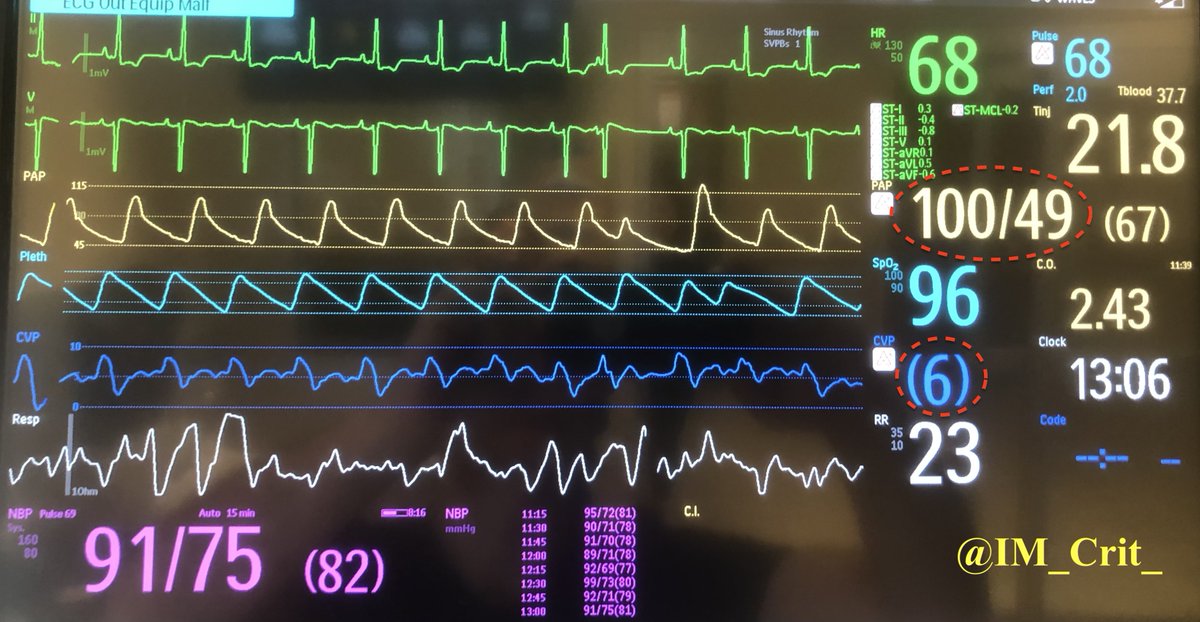
2/10) Vitals
Specifically:
Pulse pressure = SBP minus DBP. If low (<30mmHg or 40mmHg) indicator of potential low SV
RR - most useful vital for respiratory patients (and weaning)
HR - critical to diagnose etiology of shock (tachy --> ? compensatory. Brady --> ? cause)

English
I hear clinicians say the physical exam is dead.☠️ This is just not true 🛑
Here are the 10 most important clinical exam findings in the ICU
A 🧵
(and some things you can probably stop doing...)
#medtwitter #foamed

English
@IM_Crit_ Going by this algorithm, if no sustained CO2 waveform, you'd reintubate the cadaver (despite proper placement), sounds like? To me your (excellent) post reinforces the point that an important ddx to non-sustained CO2 capnography should include non-circulation or cardiac arrest.
English




@EM_RESUS Great line- though I don't think we should call them "blind" lines. They are landmark based.
English

I don’t care what anyone says, the blind subclavian central line is a very powerful one—especially in trauma. It’s becoming a lost art in the era of ultrasound, be we should never let it die.
English
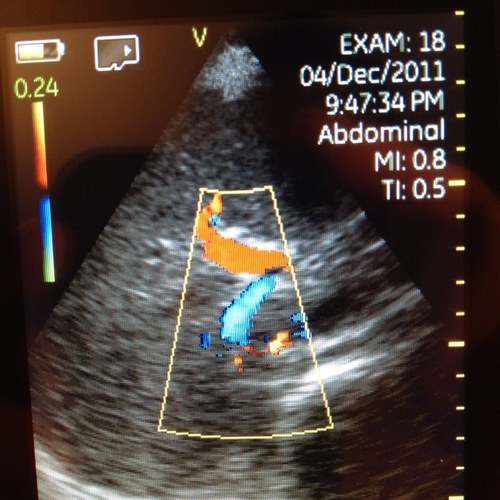
@WApplefeld @IM_Crit_ Nice breakdown. But with the calculated fick being so high, sounds like no r->l shunt?
English
@IM_Crit_ Is this some other form of shunt? Maybe a PFO that was missed throughout life and now has eisenmenger’s physiology explaining the systemic hypoxia, elevated PA pressures, and subsequently a r->l shunt?
English
Waleed Sneij retweetledi
Ten cognitive check points (general rules or heuristics to help guide my practice) I use in the ICU to help make sure I don't get too far off track. A thread🧵👇
1/10: Shock with a narrow pulse pressure (<30mmHg) needs an urgent #POCUS (or echo) to identify occult RV/LV failure, obstructive shock, or severe hypovolemia.
#medtwitter #foamed #echofirst #pocus #MedEd #medicine #FOAMcc
English
@ShahrourWalid @ranjithramamd Good questions. Probably can be a routine question put in writing for any man who gets deployed during war or even prior to such. Whether he consents to this in the event of death. Can be extended to other high risk professions, perhaps even further.
English

@ranjithramamd Interesting work. I was wondering about the ethical implications. Did this patient have their consent? What if they never wanted to father children? Etc
Thunder Bay, Ontario 🇨🇦 English
@IOHK_Charles Charles I think you should try out this amazing pizza joint!! Cardano's Pizza and Wings, in Syracuse, NY :D

English
Waleed Sneij retweetledi

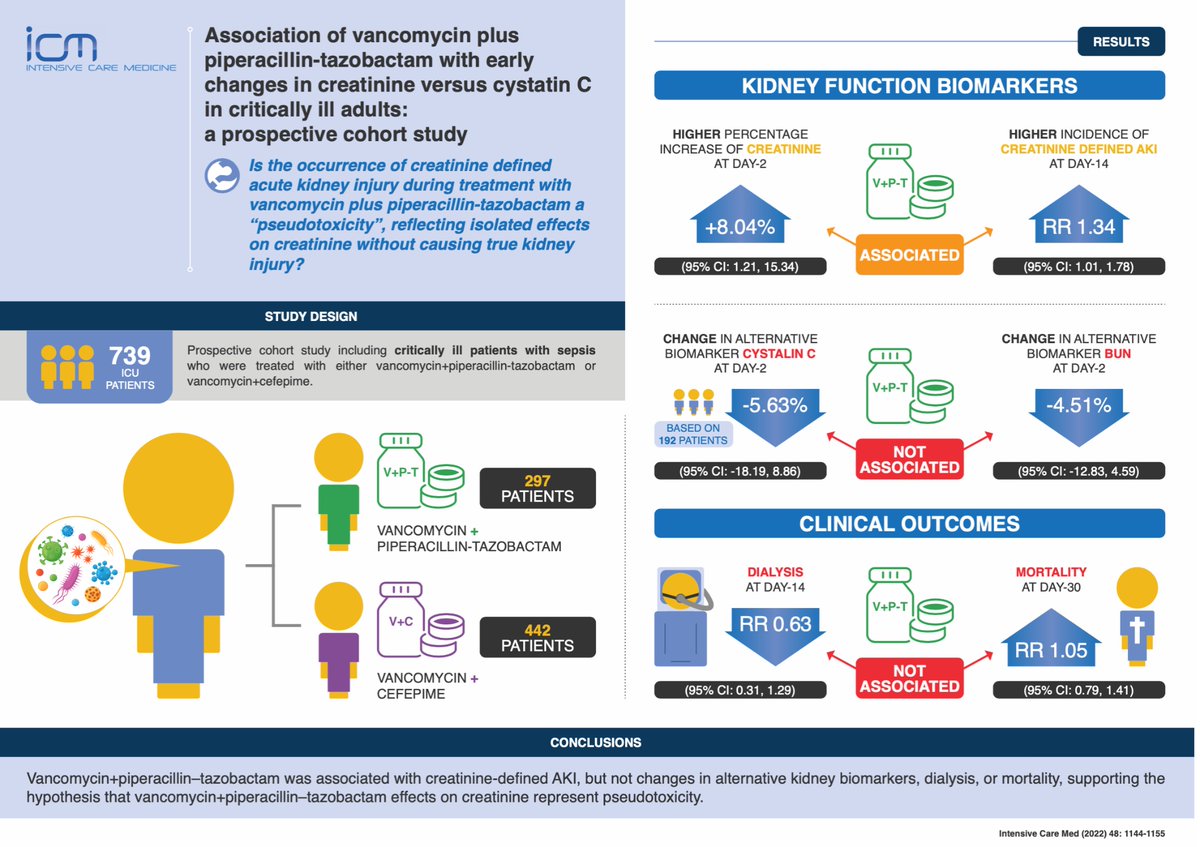
💉 Vancomycin + pip–tazo associated with ⬆️risk of creatinine-defined #AKI in critically ill: pseudotoxicity?? No changes in alternative kidney function biomarkers, nor downstream clinical outcomes associated with true AKI.
#FOAMcc
📎 rdcu.be/cRLAi
⬇️ Visual Abstract
English

Humbled and honored to be part of the most amazing team @VISN8LPOP who all wore bow ties and made a bow tie/lung cake for a surprise birthday party for me.

English
Waleed Sneij retweetledi

Can you alter the Mechanical Power in Volume Controlled Ventilation without changing the TV and RR?

English

@JacksonHealth Only liars go out of their way to say they’re numbers are accurate
English
Since March 2020, Jackson Health System has shared daily updates on the number of COVID-positive patients being treated in our hospitals, their vaccination status, and other important information that helped show a transparent,
English
Waleed Sneij retweetledi

English
English

Can ECMO cannulation primarily performed by cardiothoracic surgeons be successfully transitioned to medical intensivist-led cannulation? Explore the results of a trial that implemented this ECMO model with a new Concise Critical Appraisal: bit.ly/3m1i4uG
#SCCMSoMe
English