Kipp Johnson retweetledi
Kipp Johnson
2.6K posts


Kipp Johnson
@kippwjohnson
MD, PhD | Computational cardiology | @NU_intmed @PSTP_at_NU ex @tempusai @sinaimstp @uchicago
Chicago, IL Katılım Ocak 2014
1.4K Takip Edilen752 Takipçiler

Kipp Johnson retweetledi

this claim is always funny for 2 reasons — (1) you can’t pick a non-quantitative profession in the world more explicitly didactically trained in bayesian stats than physicians, (2) you can’t pick a group of people more interested in low PPV tests (MRI/labs/etc) than Bay Area tech
Ben Landau-Taylor@benlandautaylor
My healthcare blackpilling moment was when I was ~14, my dad explained false positive/false negative statistical tests as he drove me home, and at the end he mentioned most of his medical students never really understand how to apply the basic stuff I’d just learned.
English
Kipp Johnson retweetledi

Password rotation or Forced changes lead to "password hedging," where users just add a number or change one letter (e.g., Summer1! becomes Summer2!).
It is biologically impossible for most people to memorize a high volume of complex, random strings every few months, leading to "sticky note" security risks.
When security is a hassle, users find dangerous shortcuts, like reusing the same "strong" password across every site they own.
The most important fact is that NIST (National Institute of Standards and Technology), the global authority on cybersecurity standards, officially retired this method
In its Digital Identity Guidelines (SP 800-63B), NIST now explicitly states that organizations "SHALL NOT require" periodic password changes.
They’ve shifted the focus to Length over Complexity.
They recommend allowing passphrases of up to 64 characters and only requiring a change if there is actual evidence of a compromise.
Cyber_Racheal@CyberRacheal
Password rotation every 90 days actually makes your company LESS secure. Change my mind.
English
Kipp Johnson retweetledi

This is, imo, the most achievable and best singe answer to this question as well. the local municipalities issue is probably our single greatest. it holds back immense economic growth and general societal development.
x.com/bulkingtonbook…
Bulkington@BulkingtonBooks
@favelaoverlord here's a good one: what are policy ideas/solutions that 'China does right' that we should consider adopting/stealing for domestic use here?
English
Kipp Johnson retweetledi

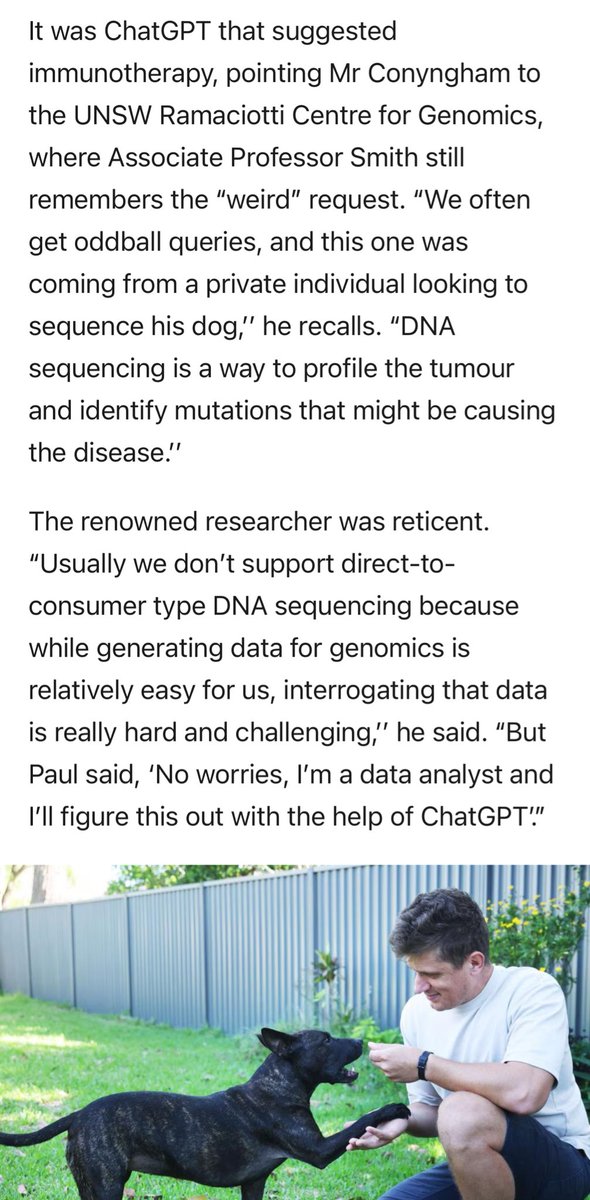
You can just do things (genetically sequence your dog’s tumors and design a bespoke mRNA cancer vaccine to save her life)

Séb Krier@sebkrier
This is wild. theaustralian.com.au/business/techn…
English
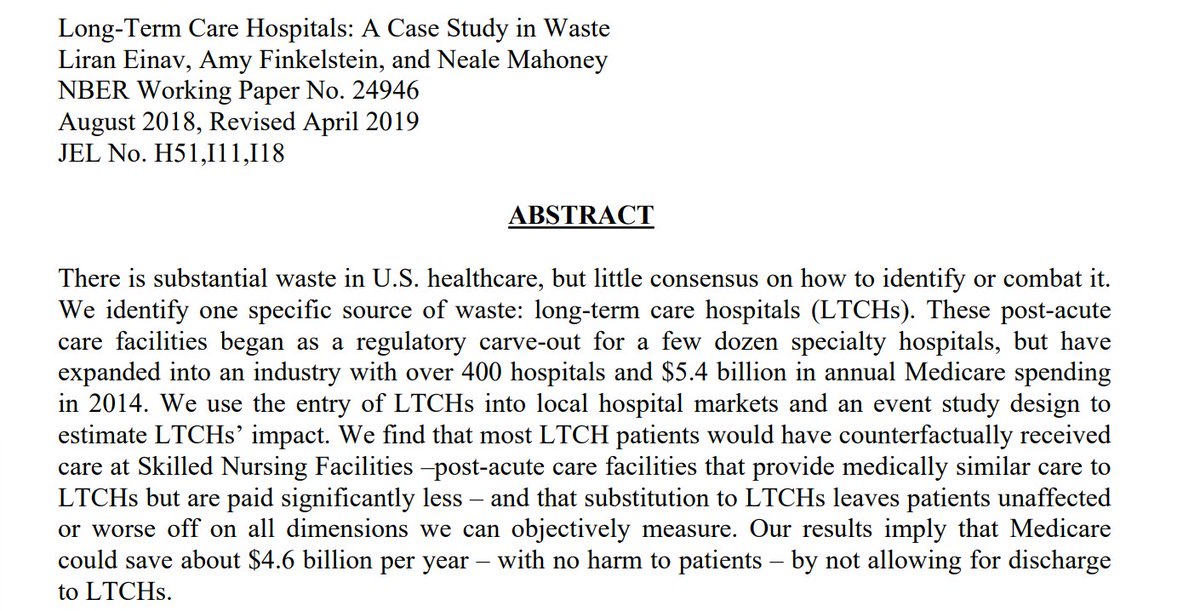
@captgouda24 @sarthakgh Long term care hospitals take care of far different patients than SNFs or SARs. Not comparable.
English

Wanna save Medicare $4.6 billion a year at no harm to the patient? Stop reimbursing long-term care hospitals three times as much for the same care provided as nursing homes! What was created as a regulatory carve-out in the 80s has grown into hundreds of wasteful hospitals. 1/
English
Kipp Johnson retweetledi

Yesterday I spent more time helping patients figure out how to pay for their medications than discussing their actual medical concerns.
This is how the souls of physicians die.
Not all at once, but one paper cut at a time.
English
Kipp Johnson retweetledi

Austin tried to pass rent control, but the state didn’t allow it. Instead, we allowed developers to build. Now it’s cheaper to rent in Austin as a % of income than in decades.
Move to states and cities that build things instead of having virtue signaling policies that don’t help
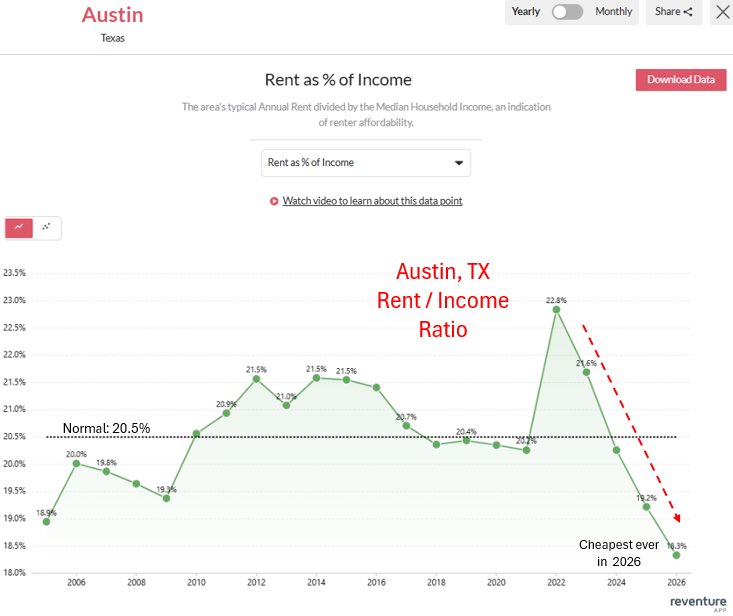
Hunter📈🌈📊@StatisticUrban
Austin, TX from the same spot 10 years apart (2014 vs 2024) Pretty stunning transformation.
English

provocative question in isolation. but then raises the questions, should residents and fellows pay for the teaching, mentorship, liability, and access to patients during training as non-licensed doctors?
Abbas M. Hassan, MD, PhD@AbbasHassanMD
Should residents & fellows bill? A single resident can provide >$300k/yr in uncompensated care due to outdated @CMSGov rules. Our @NEJM paper proposes a competency-based framework to capture this revenue, improve trainee pay, and offset massive debt. #MedTwitter #MedEd #GME
English
Kipp Johnson retweetledi

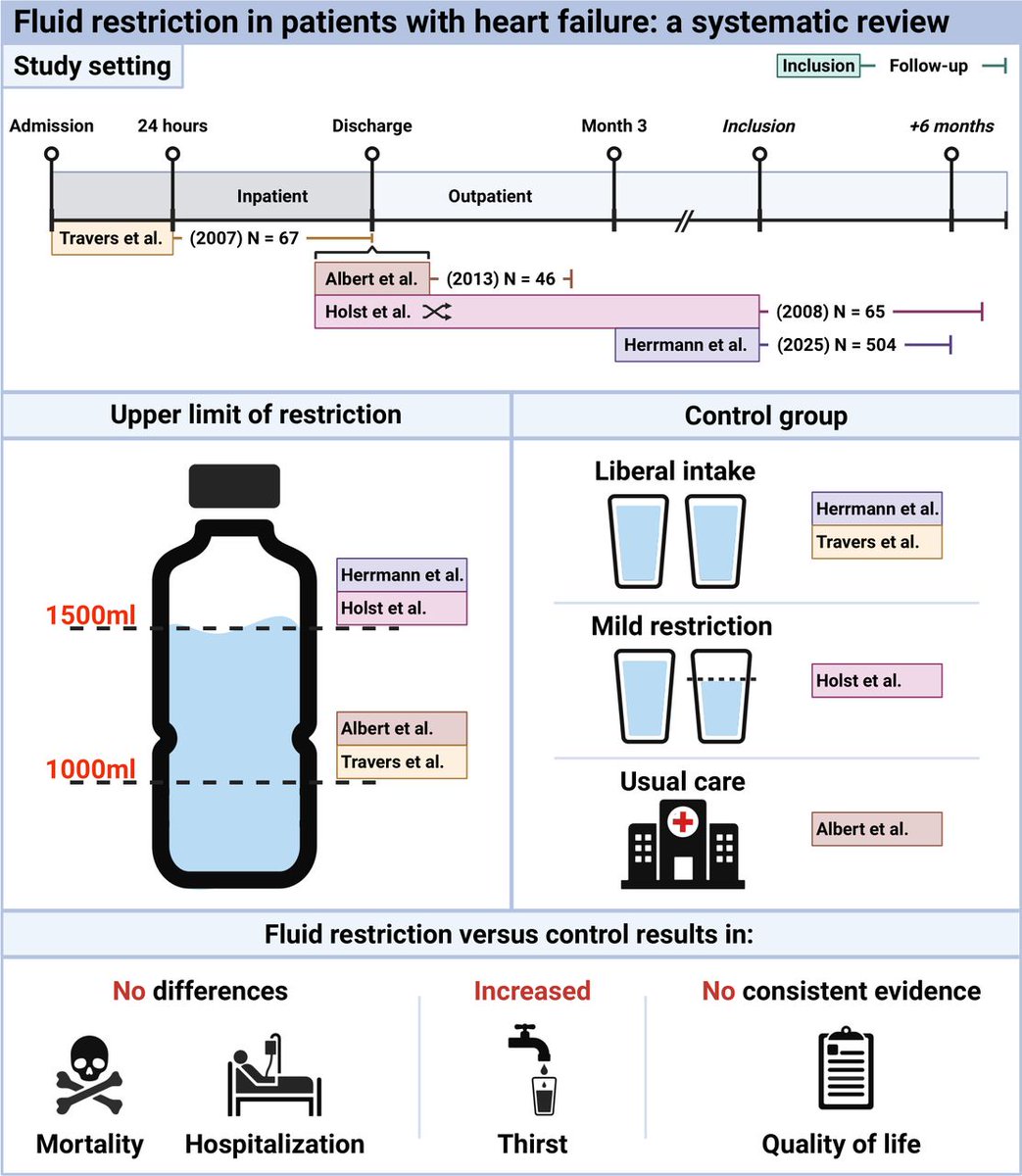
Fluid restriction in patients with heart failure: a systematic review heart.bmj.com/content/early/…
English
Kipp Johnson retweetledi

Whenever you see a contextless large number you should be pretty skeptical.
My hometown of 17,000 people uses 1.5 million gallons of water per day. Enough for 21 data centers like this. If you saw someone saying that the American west cannot afford to have 17,000 more people move there I think you'd be a little suspicious.
Irrigated alfalfa farms use about 3-4,000 gallons per acre per day, and there are 6 million acres of irrigated alfalfa in the west. That one crop (which mostly goes to feed livestock) is using as much water as 500,000 data centers at this size.
Data centers are always going to basically round to zero on the list of the west's water issues.
Benji Backer@BenjiBacker
The American West simply cannot afford to build data centers that suck up 70,000 gallons of water per day. The Western rivers are nearly dry already. And no one is talking about how bad this could get.
English
Kipp Johnson retweetledi
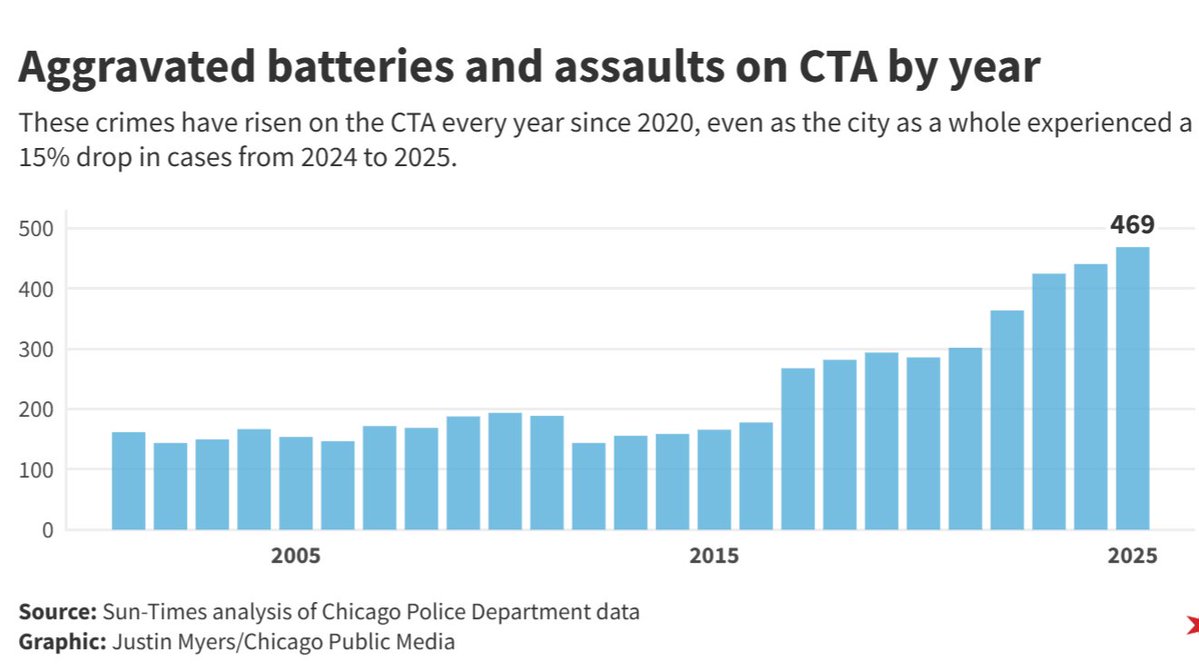
"There are more full-time police officers — an estimated 150 — on the mayor’s security detail than there are full-time police officers assigned to the CTA." — Vallas
English
Kipp Johnson retweetledi

LASIK eye surgery cost $2,200 per eye in 2000. Today it's around $1,000 per eye despite 24 years of inflation. Meanwhile, an MRI that cost $1,200 in 2000 now costs $3,000+. The difference? LASIK operates in a free market with no insurance interference and minimal regulation.
When patients pay directly, providers must compete on price and quality. LASIK clinics advertise prices, offer financing, and constantly improve technology to attract customers. Compare this to hospital procedures where prices are hidden, patients never see bills, and insurance companies negotiate opaque rates that somehow always increase faster than inflation.
Cosmetic surgery follows the same pattern. Breast augmentation, rhinoplasty, and other elective procedures have become more affordable and safer over decades. Surgeons invest in better techniques and equipment because they must satisfy paying customers, not insurance bureaucrats or hospital administrators focused on maximizing reimbursements.
The lesson is clear: remove third-party payment systems and excessive regulation, and you get Austrian economics in action. Prices fall, quality rises, and innovation accelerates. Healthcare costs aren't rising because of aging populations or new technology—they're rising because we've destroyed the price mechanism that makes markets work.
English
Kipp Johnson retweetledi

Imagine whatever your job is. Now imagine someone who has never actually done that job designs the software you are required to use to do it.
Every single task now takes an extra 50 clicks. Things that could be handled with a quick verbal order now require logging in, navigating slow pop up windows, and clicking through reminders that add nothing to the outcome.
Now imagine your inbox fills with several hundred notifications a day. Most are useless. Buried somewhere in there might be the one message that actually matters.
When you want a simple improvement to the system, you are told it has to go through layers of committees and governance meetings, only to be denied. Yet when an administrator wants to add 20 more clicks or a new mandatory alert, there is no requirement to ask the doctors and nurses who actually use the software every day.
That is what is wrong.
English
Kipp Johnson retweetledi

A very important imaging study, which a substudy of POET trial, on residual vegetations after non-surgical treatment of left-sided endocarditis.
At the end of antibiotic treatment, more than half of patients have residual vegetations on TEE. Among these patients, most vegetations are unchanged in size compared to initial TEE.
More importantly, neither the presence nor size of the residual vegetations is associated with adverse outcomes, including embolic events, up to 4 years.
jacc.org/doi/10.1016/j.…

English
Don’t sleep on circadian biology
Stephen V Liu, MD@StephenVLiu
This is a major story from #ASCO25. Randomized phase 3 trial of time of day of immunotherapy infusion. Randomized to infusion before or after 3pm. Early infusion far superior: PFS 11.3 vs 5.7 HR 0.42, OS HR 0.45! Impactful, pragmatic, not costly. This should be a bigger story.
English
Kipp Johnson retweetledi
Absolutely insane to me that a 22 year old banking analyst has stricter personal trading rules than politicians who create the law
Nancy Pelosi Stock Tracker ♟@pelositracker
Keep an eye on this one ✍️ Rep. Kevin Hern just sold off his entire $500,000 position in United Health $UNH His note in the filing was "Sell to close" Hern sits on the House Subcommittee on Health
English
@CBSSportsCFB @bmarcello This is the single dumbest and most incompetent ranking I have seen in my entire life, in any sport.
English


This is obviously not sustainable for the city
Midwest Antiquarian@Eric_Erins
“Nearly 80% of the city’s property taxes go toward pensions” Not exactly an unknown stat but it really is shocking every time you see it
English
Kipp Johnson retweetledi
“Nearly 80% of the city’s property taxes go toward pensions”
Not exactly an unknown stat but it really is shocking every time you see it
Jeanne Ives@JeanneIves
Read between the lines - Chicago is bankrupt. Only a matter of time before the layoffs start, all to pay hefty pensions of people who retired years ago with $100k+ pensions. Public Employees- your pension, your job, your home - you can't have all three. bloomberg.com/news/articles/…
English