Sabitlenmiş Tweet
Spin
1K posts


Spin
@markspin
I love markets in general and technical analysis more specifically. You’ll see me commenting on Bitcoin’s price behavior but I track a lot of different assets.
Katılım Nisan 2009
856 Takip Edilen312 Takipçiler
@jasonpizzino I’m desperately trying to be systematic with this stuff. Find rules that provide an edge. Otherwise you can be right but early or right but late or neither and it’s mental gymnastics. Right now it looks like a coin toss.
English

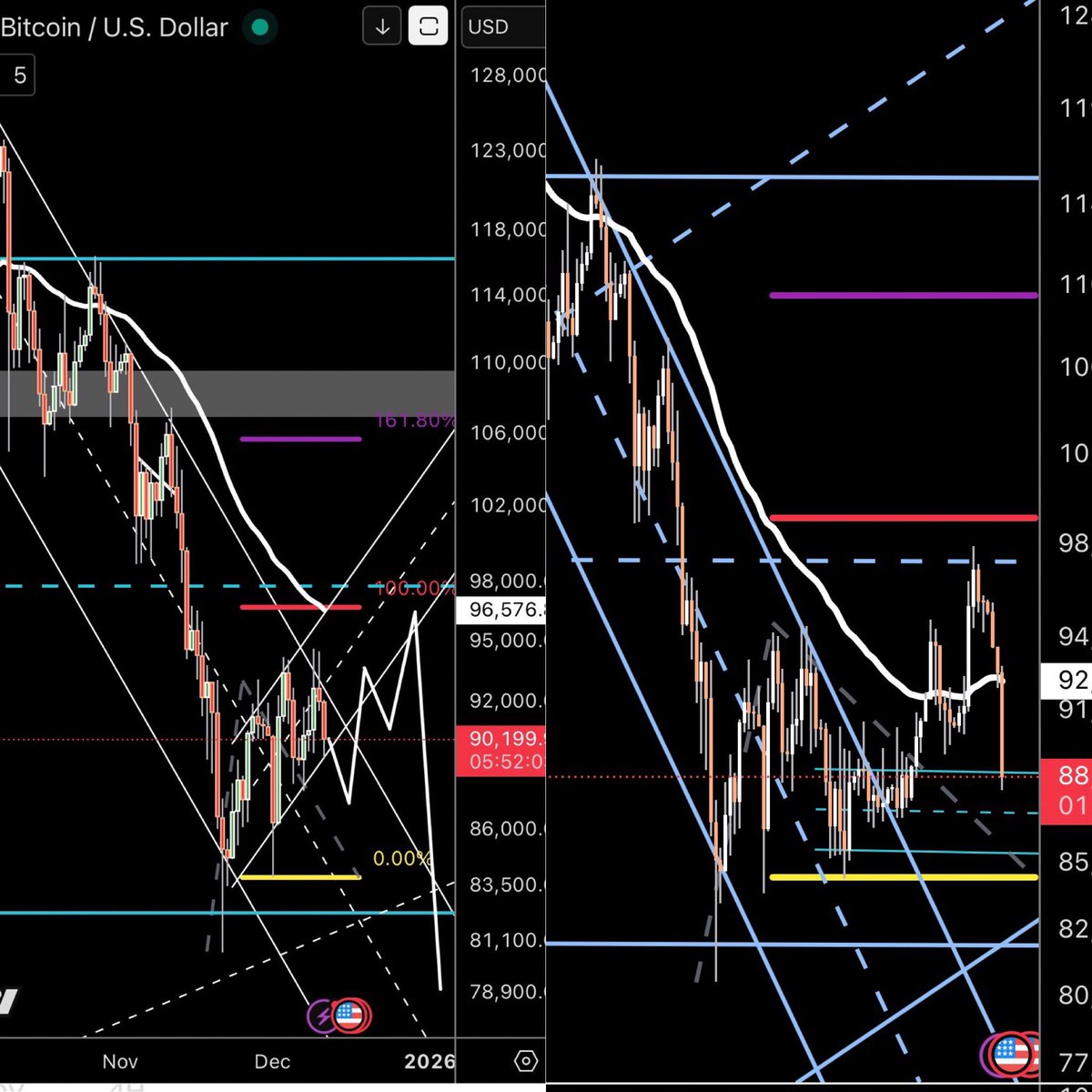
Bitcoin looks to be getting ready to test the lows again like it does every bear market (or 4-year cycle).
Falling volume, lack of social interest (search volume), and a structure reminiscent of further weakness.
The perma bears will be calling lower and lower prices, while the perma bulls will be calling it manipulation.
Don't be either. Just be prepared.

English

The only reason I’m still bear(ish), is past performance.
That’s all we have to go off of.
But going off of only a few cycles isn’t much data either.
Does it HAVE to follow past cycles? Absolutely not.
Have we broken aspects of each cycle? Yep.
Will it be a self fulfilling prophecy? Idk
But if it is….we are right here in the cycle where we typically break down further.
Let’s see what happens 🫱🏼🫲🏽

English
I don’t think anyone in their right mind would live in their car and join a gym to shower as opposed to moving to a cheaper city. Go to Houston. Come on now. What you’re saying doesn’t add up. A sober, hard working person can find work literally anywhere. Homeless people for the most part have mental issues and/or drug problems. That’s not a judgement. I say that with empathy. The truth is that it is not showing compassion to allow people to live on the street. Especially young women. What Spencer is proposing is good for the city and good for the people struggling to live there.
English

Again, I’ve worked in gyms for 20 years. I’m not generalizing anything I don’t need to look at any other source. I’m directly here in LA. I’ve been dealing with homeless people for the past 20 years because they are now smart enough to know that they can join gyms in order to shower. So I have seen all the reasons and I’m so so sorry. I know people wanna sit up on social media and overdramatize whatever is the most scandalous thing they can over dramatize today and in this case its drugs and alcohol, but sorry that is not the reason most people are on the streets.
Nobody is ignoring anything I’m going directly off of experience living here in Los Angeles.
English

NEW: Spencer Pratt fires back at reporter after he was asked about his plan for the homeless, says they will all end up in Seattle.
Reporter: "What are your plans for the over 40,000 homeless in Los Angeles?"
Pratt: "Well, they're not homeless, they're drug addicts... These people have been bused in by scam rehabs, scam NGOs, scam homeless nonprofits."
"These people, when I unplug them ... they're all going to Seattle, where the mayor will welcome them."
English
@QuintenFrancois Dips in very specific stocks and sectors. Plenty of stocks are beaten down right now.
English

Every dip in stocks now gets bought instantly like recession no longer exists as a concept
This market is fully addicted to liquidity and money printing expectations
That’s why every major crash will probably end in massive liquidity injections from governments
English
I get the logic and over time I do think it continues to go up. But if I borrowed last year when Bitcoin was $125k and now it’s $75k’ish, I’m assuming I still have to service that debt. I can’t just re-fi at a higher value and pay the loan down. I get the premise but the devil seems to be in the details.
English

@markspin @shaguncrypto The logic is that BTC goes up in value each year.
The borrower keeps borrowing against the increasingly valuable stack.
When they die, heirs inherit the BTC at current value not original cost, (stepped up value) avoiding capital gains taxes. The heirs pay off the loan.
English

You could literally -
- Stack 5 BTC at $70k ($350,000 total)
- Bitcoin reaches $1M
- Borrow just 4% against it yearly
That’s $200,000/year in liquidity
No capital gains tax & still holding the asset
Why are people still trading their Bitcoin away?
English
@Kongyiji89 @AdamBLiv What’s funny is after about 5 years of immersing myself in that info I hardly ever read about that stuff anymore. It’s almost like “once you know you just know”.
English

English

You start reading weird books.
You buy “The Bitcoin Standard” and then “The Fiat Standard” and then you accidentally end up reading Murray Rothbard, and then somehow you’re reading Mises, and then it’s 11:47 PM on a Tuesday and you’re 340 pages into “Human Action” and you’re highlighting passages about praxeology and your wife comes downstairs and asks if you’re coming to bed and you say “in a minute” but you don’t come to bed for two hours because you have just discovered that everything you were taught about economics in college was wrong, all of it, every single sentence, and now you can’t go back, you can never go back, you have been orange-pilled in a way that goes deeper than money, you have been epistemologically orange-pilled, you now believe that John Maynard Keynes was a charlatan and the gold standard was actually fine and the income tax is theft and you can never say any of this out loud at a dinner party ever again.
English

@AdamBLiv Add to that reading list; Chodorov, The Root of All Evil, The Income Twx.
English

@AdamBLiv You thought Bitcoin was an investment, but it turned out to be a doorway into questioning almost everything you were taught about money, economics, and the modern financial system.
English
@Kongyiji89 @AdamBLiv Totally agree. This is one I point to all the time. He didn’t even consider himself an “Austrian” or a “libertarian”. He’s just a logical human being who looks for evidence. God Bless Thomas Sowell.
English
@AdamBLiv To get out of the Keynesian delusion, I highly recommend Sowell’s “Basic Economics”, too, which is my favourite book. (Weird thing to have an economics book as your favourite book😂)
English
@AdamBLiv @saifedean This happened to me 15 years ago. It’s a real awakening. Unfortunately I landed on gold for the next decade after that. But the awakening is where the conviction draws from.
English

@markspin If nothing else changes (price-wise), this chart could still collapse further as the largest cohort (3-6 months) age into long-term holder status. This really could go a lot lower in the next month or so with not much happening to the price
English
Bitcoin’s short-term holder HODL Waves have collapsed.
That means the speculative dollar value sitting in weak hands has been drained from the market.
When the 0-6 month cohort shrinks into these zones, Bitcoin becomes structurally harder to dump further because there simply isn’t much hot money left to flush.
Chart → onchainmind.io

English

And now Bitcoin is impulsing.
Right off of the lows that I longed…
Whilst getting unending abusive replies on the original tweet.
I need to create a Syko tweet sentiment metric…
It would honestly be very helpful.
The more abuse I get, the more likely I’m right.
Very happy so far with a great trade.
Powered by the reply guys tears 😛

Sykodelic 🔪@Sykodelic_
I'm long. Been waiting for this level for a while now. Liquidity swept below $75,000 on a Saturday and funding has flipped negative for the first time in 6 days. Could see one more push a little lower to create some bearish divergences, but I think we hold above $73,500 and close the weekly above our key level of $74,400. We have an easy and tight invalidation here and the R/R is solid. Until we lose $74,400 on the weekly this is a HTF retest of reclaiming Bullish HTF market structure. $74,400 has been a level in my thesis for a very long time, so we want to see this hold. If we get 2x weekly closes below it I would consider that weakness and new lows would be back on the cards. But that is not what I expect.
English
@Alex4DeFi @AdamBLiv Some people are in 401k’s for 40 years. Why is this different?
English

Bitcoin is remarkably easy.
Buy it. Hold it. Never sell it.
Get disgustingly rich.
Ignore spot price. Watch the 4 year moving average.
Bitcoin only goes up and to the right.
See you all in 2030.
English
@adam3us @carlosthecomic Do you think he thought you were referring to ETH?
English



They're not going to crash the stock market. They're going to crash the dollar instead.
The Fed has done it every single time. 2008. 2019. 2020. 2023.
And they're about to do it again.
English
So you started selling $4k from the top because it wasn’t behaving the way you wanted it to? It was at all time highs basically. It ripped during the chaos of Covid. That was before gold went parabolic. Before the war. During rising interest rates. I appreciate your transparency but it doesn’t sound like a well thought out thesis.
English

Not what I said. First. I sold it before the war started. My lowest sales price was 88k. Started in the 120s.
I applied the same logic i do to stocks. If my thesis doesn't hold. Sell.
The btc thesis was that it was a hedge against diat currency failing. It was a hedge against world economic instability.
Under that logic btc should be setting new highs.
Instead it now trades as a risk on asset. That's not what btc was meant to be. At least not IMO
And who knows how much of the price is Saylor propping it up
Even the maxis haven't been as loud.
I'm not saying it goes to zero. I'm saying it's whole value is built on supply and demand, with a little premium for payments
That's not why I bought it
English

Marc Cuban sold 80% of his Bitcoin because it didn't act like a hedge during the Iran war.
Gold hit $5,000. BTC dipped. He called it a disappointment and walked.
But BTC is up 16%+ since the conflict started.
He measured a 4-year asset by a 4-week window.
That's not analysis. That's impatience.


English

@World_Warrior @Rothmus So, you are suggesting that the Native Americans should not have fought against us and just let us take over?
English

This is a major reason why mass immigration generates such intense resentment.
Many immigrants not only fail to identify with their new country and its native people, but they actively oppose them and everything the host culture represents.
Here she is, the same person defines “ethnic cleansing” as the permanent resettlement of an entire ethnic group from their homeland, yet openly celebrates the demographic decline of the white British population, declaring “We are winning.”
This isn’t treason. Treason implies betrayal from within a group.
This is something else entirely: a demographic invasion by people who were never part of the historic British nation. An ethnic cleansing per her own definition.
When native Britons say “send them all back,” it’s really hard not to sympathize.
English