
Rob Douglas
37.6K posts
Rob Douglas
@RobDouglas
ID Theft & Fraud Prevention Consultant ~ Aspiring Gym Rat ~ Fmr Private Detective ~ Fmr Political Commentator ~ Student of Stoicism ~ Disciple of Nature
Colorado, USA Katılım Ekim 2009
1.7K Takip Edilen2.5K Takipçiler

Thomas Massie is a goddamn American hero.
You’ll never convince me otherwise. And some of you should feel very ashamed.
English
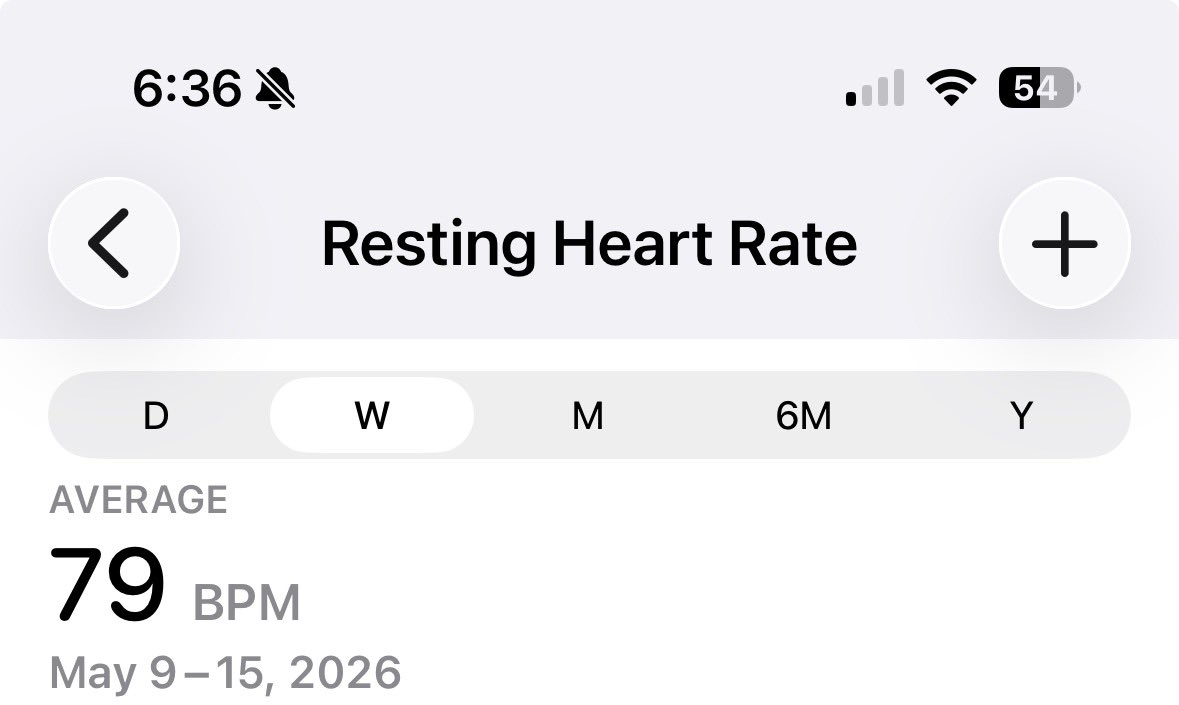
My RHR has now dropped from the upper 80s into the 70s. Next goal is to get it down into the 60s. I suspect 5 days/week strength training, and some form of cardio every day is paying off.
English
Rob Douglas retweetledi

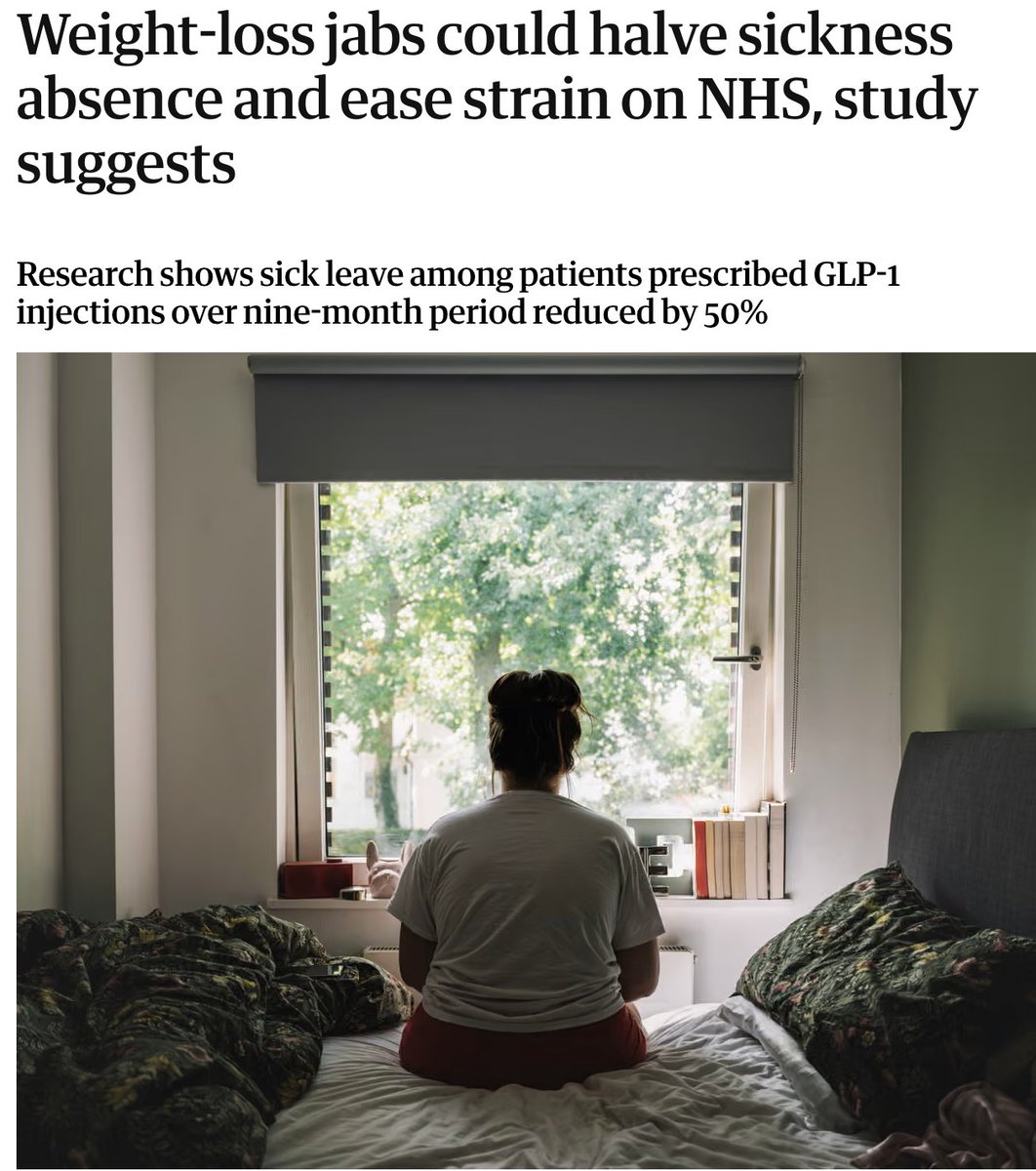
GLP-1s are associated with:
45% fewer sick days
56% fewer longer sickness absences
43% fewer in-person GP visits
48% fewer remote GP visits
25% fewer ED visits
12.4% average weight loss over 9 months
There's never been a drug like this before.
English
If you’re interested in peptides, this is a must-read post by the founder of @healthspanmed about a just-released, bombshell report on research that may vastly expand the universe of peptide therapy. The report is attached to Daniel’s post.
Daniel Tawfik@dantawfik
The human proteome just expanded by thousands of proteins—and most of them are sized perfectly for peptide therapeutics. A new Nature study from the TransCODE Consortium analyzed 95,520 proteomics experiments and found that approximately 25% of 7,264 non-canonical open reading frames encode detectable microproteins in human cells. These sequences produce peptides ranging from 8 to 100 amino acids. That's the therapeutic window where synthetic peptides can be manufactured, modified for stability, and delivered as drugs. Peptide therapeutics have been constrained by the need to target biologically active sequences that are small enough to synthesize but specific enough to produce therapeutic effects. The challenge has been identifying which endogenous peptides perform essential cellular functions and which can be modified into pharmacologically stable molecules. This study systematically maps thousands of naturally occurring peptides that cells translate and use across tissues and disease states. Many were detected in the HLA PeptideAtlas—240 million mass spectrometry spectra from immunopeptidomics datasets showing which peptides cells present on their surface. That's direct evidence of biological relevance. Cells don't randomly present peptides on HLA molecules. Presentation indicates processing, translation, and integration into cellular signaling or immune surveillance. The therapeutic implications operate across multiple modalities. First: peptide replacement therapy. If microproteins perform essential cellular functions but decline with age or disease, synthetic versions could restore activity. This mirrors the logic behind hormone replacement—when endogenous production drops, exogenous supplementation compensates. The consortium demonstrated that one peptidein from the OLMALINC long non-coding RNA produces a pan-essential cellular phenotype. CRISPR screens showed its loss disrupts fundamental processes. That's a candidate for peptide replacement if expression declines in specific tissues or aging contexts. Other microproteins may regulate mitochondrial function, proteostasis, or cellular senescence. If age-related decline in these peptides contributes to metabolic dysfunction, peptide-based interventions could target those pathways directly rather than modulating upstream regulatory machinery. Second: peptide antagonists. Some microproteins may drive pathological processes—inflammatory signaling, oncogenic pathways, or maladaptive stress responses. Designing antagonist peptides that block microprotein activity creates therapeutic options for conditions where microprotein overexpression or dysregulation contributes to disease. The study found cancer-specific microproteins expressed in malignant cells but not normal tissues. These represent targets for peptide-based inhibitors that disrupt cancer cell signaling without affecting healthy cells. Because these sequences aren't part of the canonical proteome, conventional small molecule screens wouldn't have identified them. Third: peptide vaccines. The HLA PeptideAtlas detected peptides from 1,785 ncORFs presented on cell surfaces. Cancer cells presenting unique microprotein-derived peptides expose targetable antigens for therapeutic vaccines. This approach already exists with neoantigens—tumor-specific mutations that generate novel peptides recognized by T cells. Microprotein-derived peptides expand that target space. They're not mutations—they're translation products from sequences that normal cells suppress but cancer cells express. Peptide vaccines could train the immune system to recognize and eliminate cells presenting these cryptic antigens. Because microproteins are often cancer-restricted, this strategy may produce stronger anti-tumor responses with fewer autoimmune risks than vaccines targeting overexpressed canonical proteins. Fourth: cell-penetrating peptides and delivery vehicles. Some microproteins may function as endogenous cell-penetrating sequences—naturally occurring peptides that cross membranes or localize to specific organelles. Identifying these sequences could improve drug delivery technology. Current peptide therapeutics face bioavailability challenges. Oral delivery is difficult due to enzymatic degradation. Systemic delivery requires modifications to extend half-life and prevent renal clearance. Intracellular targeting remains complex because most peptides don't efficiently cross lipid bilayers. If evolution has already produced microproteins with membrane-crossing or organelle-targeting capabilities, those sequences could be incorporated into therapeutic peptides to improve cellular uptake and subcellular localization. Fifth: synthetic biology and designed peptides. The study provides a catalog of naturally occurring bioactive peptides that cells translate and tolerate. That catalog becomes a training set for designing synthetic peptides with desired pharmacological properties. Machine learning models trained on microprotein sequences—combined with data on their tissue expression, HLA presentation, and evolutionary constraint—could predict which synthetic peptide sequences will be stable, non-immunogenic, and biologically active. This accelerates peptide drug development by narrowing the design space. Rather than screening random sequences, developers can modify known functional microproteins or generate synthetic analogs based on evolutionary patterns. The manufacturing advantage: peptide synthesis is straightforward. Unlike biologics requiring expression systems and purification pipelines, peptides can be chemically synthesized at scale. Modifications to enhance stability—D-amino acids, cyclization, lipidation—are well-established. The pharmacokinetic challenge has been specificity and half-life. Endogenous microproteins solve the specificity problem—they're already performing targeted cellular functions. Engineering modifications to extend circulation time becomes the primary optimization. The evolutionary analysis supports therapeutic viability. The consortium developed ORF relative branch length (ORBL) to measure selective constraint on microproteins. Sequences under purifying selection across mammalian evolution are preserved because they perform functions that natural selection maintains. That's evidence these peptides matter biologically. Therapeutic interventions modulating microprotein activity aren't targeting random noise—they're engaging functional molecules shaped by millions of years of selection pressure. The annotation framework enables systematic peptide therapeutic development. By formalizing peptideins as a recognized classification in GENCODE and PeptideAtlas, the consortium creates searchable databases where researchers can identify microproteins relevant to specific diseases, tissues, or cellular processes. Pharma companies developing peptide therapeutics can now query: which microproteins are dysregulated in this disease? Which are cancer-specific? Which show tissue-restricted expression? Which are presented on HLA in patient samples? Those queries weren't possible when microproteins remained unannotated. Now they're part of the reference proteome. The clinical development timeline depends on functional validation. Demonstrating that a microprotein performs a therapeutically relevant function—and that modulating it produces measurable clinical benefits—requires the same rigor as conventional drug development. But the discovery phase just accelerated. Instead of screening millions of synthetic peptides for activity, researchers can start with endogenous sequences that cells already use. The study detected 183 ncORFs with high-confidence peptide evidence in conventional samples and 1,785 in HLA immunopeptidomics. That's thousands of potential therapeutic leads—some for replacement, some for antagonism, some for immune targeting. The immediate research agenda involves characterizing which microproteins show disease-specific expression patterns, which can be chemically synthesized with therapeutic stability, and which produce pharmacological effects when administered exogenously. The decisions about which microproteins to develop as therapeutics will depend on target validation showing that the peptide performs a function relevant to human disease and that synthetic versions can recapitulate or block that function. Peptide therapeutics have been limited by the need to find biologically relevant short sequences. This study just mapped thousands of them.
English
I’d bet the fortune I don’t have that much of my success over the last seven months comes down to one thing: refusing to treat weekends like a vacation from health and fitness discipline. For me, it would be counterproductive to grind for five days, then spend two days undoing the ground I gained. The way I see it, progress doesn’t care what day it is.
English
Exercising my right thumb by clicking the Block button to eradicate nitwits and morons from my timeline is my favorite workout of the day.
English
For those trying to build or maintain an audience on this platform >>>
English
Upper 2 (Back+) at the local gym is done. PRs on all exercises, so the weight goes up again next rotation. Just had a post- workout meal plus I had pre- and post-workout aminos. Tomorrow is an extra arms workout in my home gym.

English
@DigitalFringed1 @DoNotComply23 In the case of @DigitalFringed1 it was because, unbeknownst to anyone, Guinea Pigs know how to file complaints on X.
English

@DoNotComply23 They hate people with the best takes and fizeeks. Nothing else makes sense.
English

H2K is having issues…
Why is Twitter like this?? It’s like they’re shadow banning people. It happened to @DigitalFringed1 not long ago too.
H2KMFer@H2KMFer
@DoNotComply23 I can comment and like but not post!
English
Truth. Randy goes above and beyond. I live in the far northwest corner of Colorado. I am literally in the last neighborhood that UPS and FedEx get to on any given day, and along with the USPS, many deliveries take additional days. Randy was kind enough to upgrade me to overnight deliveries at no additional cost.
English

Yeah, then when the test doesn’t pan out, many say “use Janoshik,” which is expensive and in Europe. Then if they do refund or reship, it’s just the cost of the product, not the cost of the test. It’s a giant pain. We ship same day, and as @RobDouglas can attest, we’ll even upgrade to overnight if they live in a rural area where the mail sucks.
English
Krysia does a tremendous job chronicling the horrors many experience buying peptides direct from China. It’s not for the faint of heart.
For those that want to buy direct from China, waiting weeks for delivery, weeks more for testing, saving some coin if it tests well, being our a lot of money (at least the several hundred dollar testing cost) if it fails, give her a follow first.
Krysia@Krysia830073
We have another kit with yet another new label that testing has shown tirzepatide not Reta. Someone called Yula is the vendor.
English
If it’s Friday, it’s Upper 2 - Back+. Time to fuel up and go have fun at the gym.

English
Exactly. Think of food as only fuel needed to get healthy. Replace so-called comfort food with comfort activities. A good long walk in nature. Exercise that will give you the dopamine hit you used to get from food. Do activities out of the house and away from food. You’re on the right path!!
English

Reminder: this is just me journaling.
Almost therapeutic honestly. I’m sharing it in hopes that if someone starts a GLP journey, they can read my entries and feel less alone.
I went into this knowing the mental side would be a huge piece.
But I didn’t realize how fast I’d have to adapt.
Unlike Ozempic, on reta I noticed food doesn’t really give me that same rush. I eat and it’s just… food. No big dopamine hit.
The first few weeks I still had “cheat” weekends, but even then I ate way less. Looking back, it was mostly just out of habit.
So I had to change the way I look at food quickly.
Instead of getting down about something that’s been emotional support for me since I was a kid, I’m trying to reframe it.
If food isn’t giving me that rush anymore, I might as well treat it like fuel.
And honestly? I’m okay with that.
I’ve had way too much fun with food for most of my life. I’m okay taking a break.
Because I badly want change.
Enjoy your Friday. Weigh-in day tomorrow.
-Patient023
#Retatrutide #GLP1 #FoodNoise #WeightLossJourney #SelfImprovement
English
@DigitalFringed1 That looks delicious. I eat berries and no fat yogurt for breakfast. Gonna try adding angel food cake.
English
As you all know, my fav thing in the world is cake
I also eat Greek yogurt multiple Xs a day
Someone pointed out that I should put Angel food cake in my Greek yogurt
0g of fat and pure deliciousness
How did I not think of this!!!!!

English
I must agree with my coach here. I have learned that if I consume a healthy portion of carbs both before and after my workouts, they are a significant benefit. Since I started following Leo’s advice on how to structure my macros to certain times of day, I can eat more than I ever did on any “diet,” still lose weight, and increase my strength in the gym.
SilverFoxLeo@BowTiedHRT
If you’re trying to build your physique, lose fat, or simply improve your cognitive and physical performance, not to mention increase your work capacity, and you’re doing anything remotely close to low-carb, you are sabotaging yourself. Intermittent fasting is absolute garbage. You’re just using the clock to reduce your calorie intake and simultaneously torpedoing your metabolic health and performance. Keto, outside of those who’ve made the prior commitment to becoming metabolically fluid, is absolute garbage. And anything low-carb outside of those with severe metabolic disorders or insulin resistance is absolute garbage as well. Carbohydrates are the cleanest fuel you can run on. Carbs refill muscle glycogen, which is what actually powers a hard training session, and they keep your central nervous system fed so your output in the gym and your output at work both stay sharp. Fat and ketones can keep you alive. Carbs let you perform. Eat more carbohydrates. Time your macros properly. But don’t deprive yourself of the finest form of energy you can feed yourself with.
English
@BowTiedHRT Thank you!! I think the TRT protocol you’ve designed for me is greatly helping. My recovery seems faster and I’m adding weight to each exercise most every time. Take a peek at the DM I just sent when you have a moment. And have a great weekend, coach!!
English

@RobDouglas Heck yeah Rob!! Loving the training and progress log you’re putting together here.
English
Friday week check-in!
This week I feel like I’ve been on cruise control. Laser focused.
It’s crazy how dialed in you can get when the food noise gets turned down and you’re not battling yourself all day.
It’s like trying to drive with someone screaming directions in your ear nonstop… and then suddenly the car goes quiet.
You can finally just drive.
Only real downside this week was some acid reflux.
Gym was solid too:
• Push
• Pull
• Legs
• Upper
• Lower
If anyone has gym split suggestions, I’m all ears.
Tomorrow is weekly weigh-in day and I’m excited to see how the May challenge is showing up on the scale.
Locked in.
-Patient023
#Retatrutide #GLP1 #WeightLossJourney #FoodNoise #GymProgress
English

Are we living longer?
Or are we dying longer?
English
One day at a time, Dave. I started on October 7 of last year. I’m down 97. Have at least another 60 to go. I only think about today. Never yesterday or tomorrow. What are my health and fitness goals for today. What is my food plan for today. What is my workout for today. What is my cardio for today. If I do that, I know the weekly and monthly trends will take care of themselves. Stick with Dean and you’ll learn will have success and be proud of yourself!
English

@DeanTTraining @RobDouglas I think if I had 10-15 lbs to lose I might think differently…but I am still close to 80-90lbs overweight or more. But I do recognize that I should be less afraid of the number than I currently am.
English

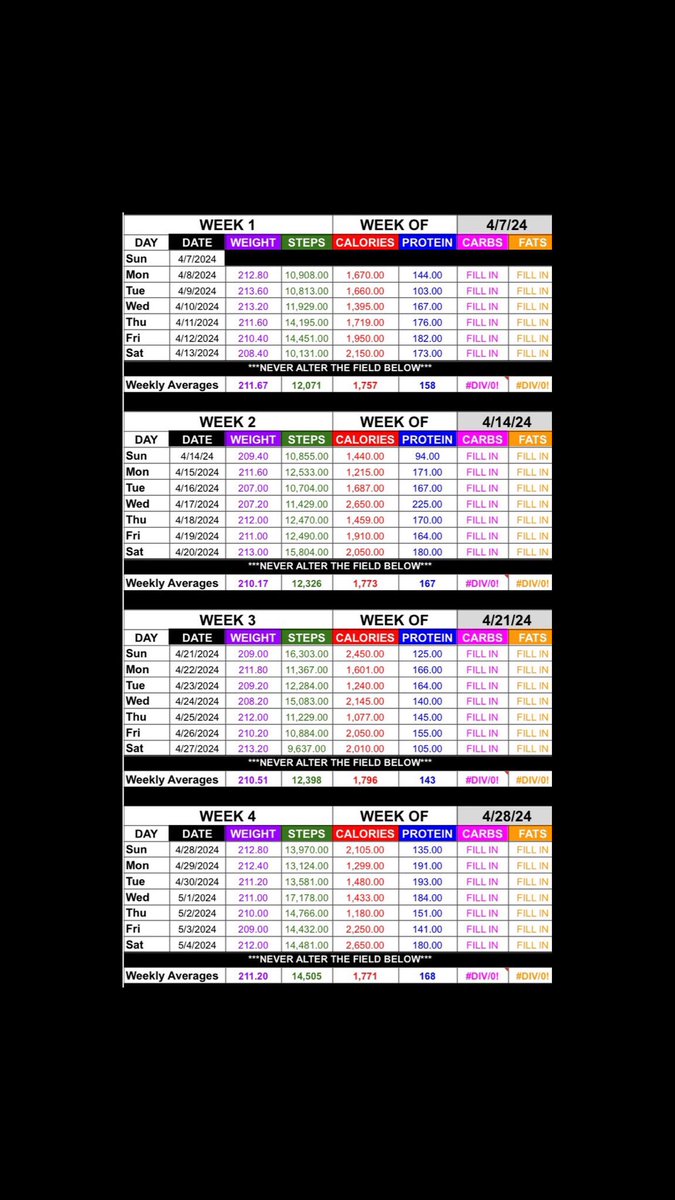
I once had a client who swore up and down he was eating < 1,800 calories per day
Steps were 12,000+ per day & he weighed ~211 lbs
His weight was basically stagnant for 1 full month
The math was NOT mathing
I intervened by hand creating a diet for him that hit 1,800 calories per day almost exactly & told him “eat only this”
Lo and behold:
He goes from 211 to 201 over the next 5 weeks
You’d be SHOCKED at how common this is in the training/coaching realm

Mario Tomic@mariotomich
29 out of 30 obese men claimed they ate ~2500 kcal while actually eating ~4000 kcal a day. They were off 37%, ~1500 kcal. Enough to lose 3 lbs per week. Even when they knew they were being watched, they still underreported almost 500 kcal per day. The first step to losing fat is facing the truth about your intake and tracking your calories. If you can't do that, everything else fails.
English